

Using Nicotine Gum to Assist Nondaily Smokers in Quitting: A Randomized Clinical Trial
- PMID: 31125988
- PMCID: PMC7297094
- DOI: 10.1093/ntr/ntz090
Using Nicotine Gum to Assist Nondaily Smokers in Quitting: A Randomized Clinical Trial
Abstract
Introduction: Non-daily intermittent smokers (ITS) comprise 30% of US adult smokers. ITS smoke for nicotine and have trouble quitting, but tend to smoke in particular situations. This study tested the effect of nicotine gum, used to prevent or react to situational temptations, for helping ITS quit.
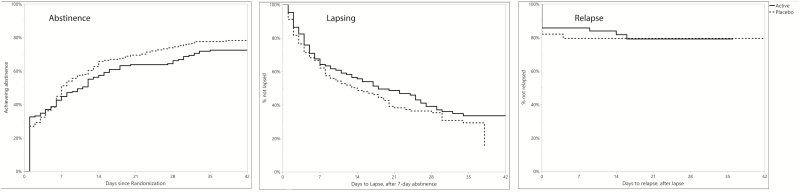
Methods: ITS (smoking 4-27 days/month) seeking help quitting were randomized to 2 mg nicotine gum (n = 181) or placebo (n = 188), to be used to anticipate or react to temptations to smoke, for 8 weeks. Participants received up to six sessions of behavioral counseling. The primary outcome was 6-month biochemically verified continuous abstinence; analyses also examined 14-day point-prevalence abstinence at multiple time points, and used event-history analyses to assess progression to abstinence, lapsing, and relapsing. Analyses adjusted for group differences in age and baseline smoking, and considered several potential moderators of treatment effects.
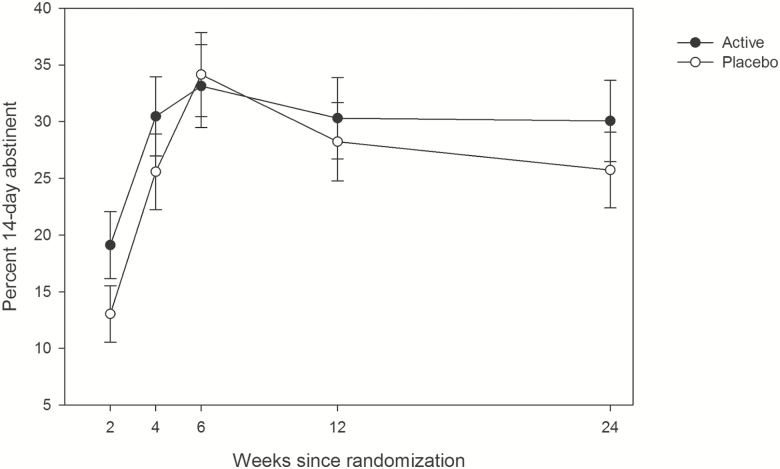
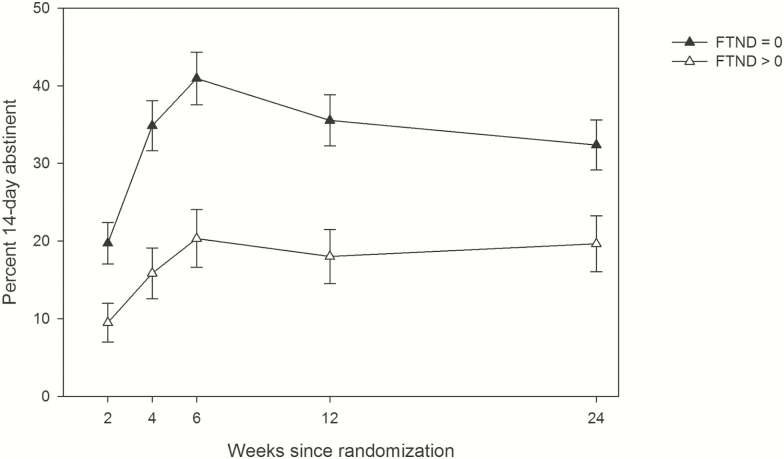
Results: Nicotine gum did not significantly improve outcomes on any measure. Biochemically verified 6-month continuous abstinence rates were 7.2% for active gum and 5.3% for placebo (AOR = 1.39, 0.58-3.29, p > .25). ITS with any degree of dependence (Fagerstrom Test of Nicotine Dependence scores >0) showed poorer outcomes on multiple endpoints, and did more poorly on active gum on some outcomes. Gum use was low, starting at 1 gum per day on average and declining over time.
Conclusions: Nicotine gum (2 mg), used intermittently, did not improve cessation rates among ITS, including those demonstrating some degree of dependence.
Implications: Nicotine replacement has been extensively tested with daily smokers, especially those who smoke relatively heavily. Nondaily smoking is now common, creating a need for treatment for ITS. Despite evidence that ITS' smoking is motivated by nicotine-seeking, a theoretically and empirically derived situational approach to using acute nicotine replacement was not successful at helping ITS quit. Gum use was low; whether higher or more frequent dosing is needed, or whether an entirely different approach is needed, is not clear. Effective treatment options are needed for ITS, especially those with some degree of dependence.
© The Author(s) 2019. Published by Oxford University Press on behalf of the Society for Research on Nicotine and Tobacco. All rights reserved.For permissions, please e-mail: journals.permissions@oup.com.
Figures
Similar articles
-
Safety and efficacy of the nicotine patch and gum for the treatment of adolescent tobacco addiction.Pediatrics. 2005 Apr;115(4):e407-14. doi: 10.1542/peds.2004-1894. Pediatrics. 2005. PMID: 15805342 Clinical Trial.
-
Quitting by gradual smoking reduction using nicotine gum: a randomized controlled trial.Am J Prev Med. 2009 Feb;36(2):96-104.e1. doi: 10.1016/j.amepre.2008.09.039. Am J Prev Med. 2009. PMID: 19135903 Clinical Trial.
-
Effectiveness of nicotine gum in preventing lapses in the face of temptation to smoke among non-daily smokers: a secondary analysis.Addiction. 2020 Nov;115(11):2123-2129. doi: 10.1111/add.15083. Epub 2020 May 14. Addiction. 2020. PMID: 32285979 Clinical Trial.
-
A review of the efficacy of smoking-cessation pharmacotherapies in nonwhite populations.Clin Ther. 2008 May;30(5):800-12. doi: 10.1016/j.clinthera.2008.05.010. Clin Ther. 2008. PMID: 18555928 Review.
-
Sex differences in long-term smoking cessation rates due to nicotine patch.Nicotine Tob Res. 2008 Jul;10(7):1245-50. doi: 10.1080/14622200802097506. Nicotine Tob Res. 2008. PMID: 18629735 Review.
Cited by
-
Smoking Cessation Smartphone App for Nondaily Smoking With Telephone Onboarding: Proof-of-Concept Randomized Controlled Trial.JMIR Mhealth Uhealth. 2025 Jan 15;13:e53971. doi: 10.2196/53971. JMIR Mhealth Uhealth. 2025. PMID: 39814363 Free PMC article. Clinical Trial.
-
Prevalence and Trends in Cigarette Smoking With and Without Tobacco Use Disorder Among Adults in the United States: 2010-2021.J Clin Psychiatry. 2024 Jun 12;85(3):23m15086. doi: 10.4088/JCP.23m15086. J Clin Psychiatry. 2024. PMID: 38874573 Free PMC article.
-
Testing the Outcomes of a Smoking Cessation Smartphone App for Nondaily Smokers: Protocol for a Proof-of-concept Randomized Controlled Trial.JMIR Res Protoc. 2023 Feb 14;12:e40867. doi: 10.2196/40867. JMIR Res Protoc. 2023. PMID: 36787172 Free PMC article.
-
Factors Associated With Cannabis Use Among African American Nondaily Smokers.J Addict Med. 2020 Sep/Oct;14(5):e170-e174. doi: 10.1097/ADM.0000000000000652. J Addict Med. 2020. PMID: 32187115 Free PMC article. Clinical Trial.
-
Very Light Daily Smoking in Young Adults: Relationships Between Nicotine Dependence and Lapse.Nicotine Tob Res. 2021 Jan 22;23(2):327-333. doi: 10.1093/ntr/ntaa169. Nicotine Tob Res. 2021. PMID: 32877533 Free PMC article.
References
-
- Stolerman IP, Jarvis MJ. The scientific case that nicotine is addictive. Psychopharmacology (Berl). 1995;117(1):2–10; discussion 14. - PubMed
-
- Benowitz NL. Clinical pharmacology of nicotine: Implications for understanding, preventing, and treating tobacco addiction. Clin Pharmacol Ther. 2008;83(4):531–541. - PubMed
-
- Babb S, Malarcher A, Schauer G, Asman K, Jamal A. Quitting smoking among adults – United States, 2000-2015. MMWR Morb Mortal Wkly Rep. 2017;65(52):1457–1464. - PubMed
-
- Stead L, Perera R, Bullen C, et al. . Nicotine replacement therapy for smoking cessation. Cochrane Database Syst Rev. 2012;11(CD000146). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
