

Functional and morphological results of treatment of macula-on and macula-off rhegmatogenous retinal detachment with pars plana vitrectomy and sulfur hexafluoride gas tamponade
- PMID: 31126280
- PMCID: PMC6534838
- DOI: 10.1186/s12886-019-1120-3
Functional and morphological results of treatment of macula-on and macula-off rhegmatogenous retinal detachment with pars plana vitrectomy and sulfur hexafluoride gas tamponade
Abstract
Background: To examine morphological and functional results after pars plana vitrectomy (PPV) with sulfur hexafluoride (SF6) gas tamponade due to macula-on and macula-off rhegmatogenous retinal detachment (RRD) during 6 months of the follow-up.
Methods: The study included 62 eyes that underwent successful PPV with SF6 tamponade with macula-on (34 eyes) and macula-off (28 eyes) RRD preoperatively. The best-corrected visual acuity (BCVA), Amsler test, M-charts, optical coherence tomography (OCT) and microperimetry were performed at 1, 3 and 6 months postoperatively.
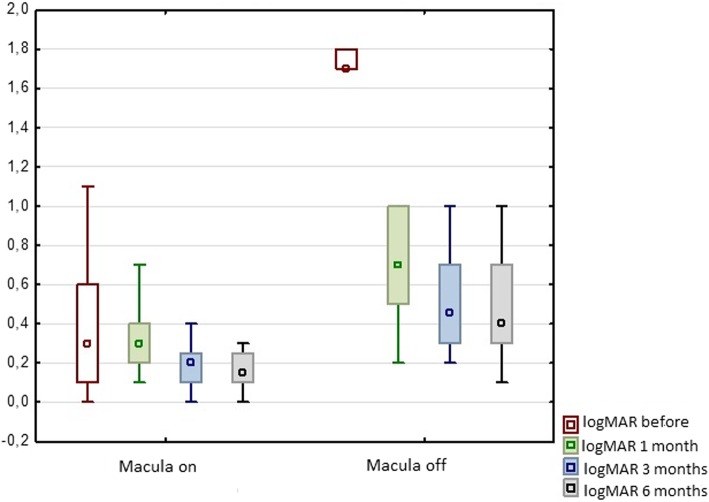
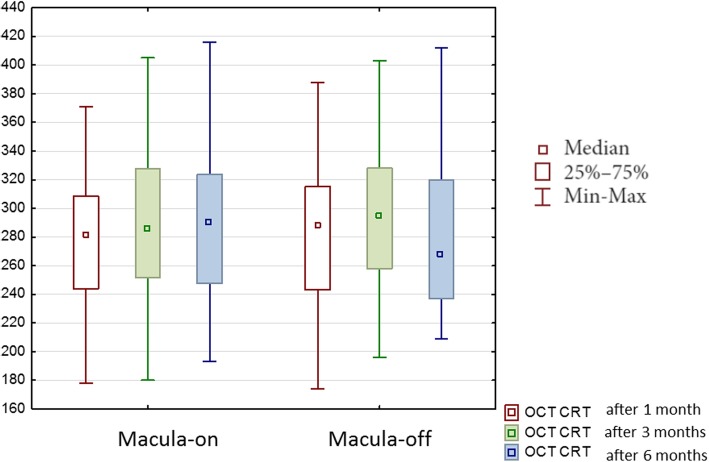
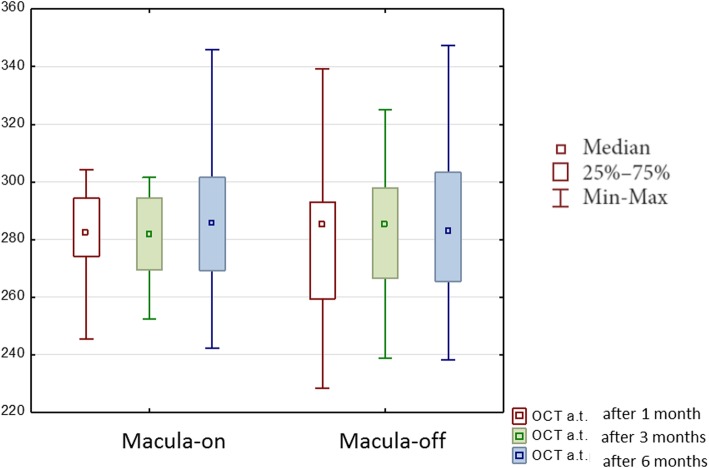
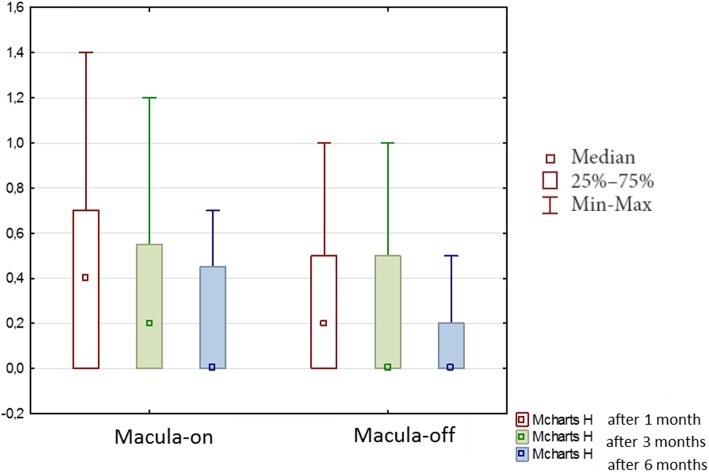
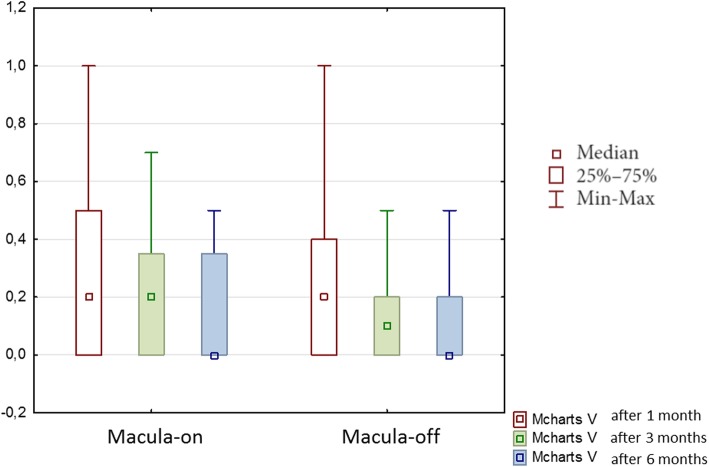
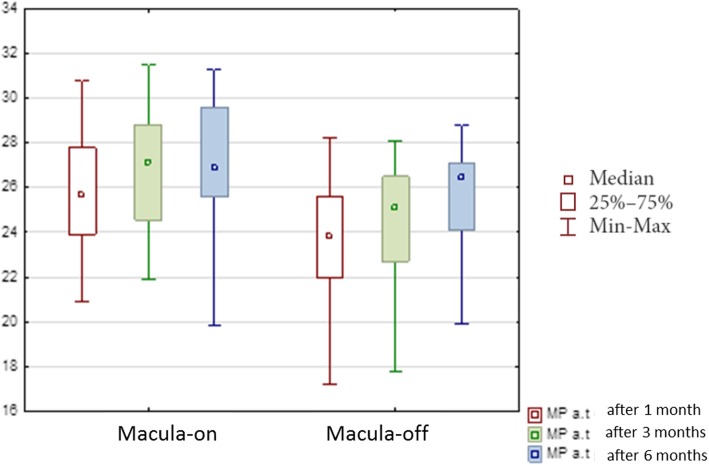
Results: Results of the Amsler test were abnormal postoperatively in 54% of the patients in the group with macula-off and in 32% of the patients with macula-on RRD. Horizontal M-charts improved significantly from 0.33 to 0.2, vertical M-charts- from 0.29 to 0.17 during 6 months of the follow-up. There was a significant increase in the central retinal thickness (CRT) and average thickness (AT) between follow-up examinations only in the macula-off group. 29 of 62 eyes (47%) after surgery (equally with macula-on and macula-off RRD) showed morphological changes in OCT in the macular region, as epiretinal membrane, macular edema, subretinal fluid or alterations of the outer layers of the retina. The average threshold in microperimetry increased significantly within both groups during the follow-up.
Conclusion: Both horizontal and vertical M-charts scores, as were as microperimetry sensitivity improved significantly during the 6 months of the follow-up both in macula-on and macula-off group. Although PPV with SF6 gas tamponade was successful, almost half of eyes revealed anatomical changes in the macular region in OCT both with macula-on and macula-off group.
Trial registration: Current Controlled Trials NCT03902795 registered on 03/04/2019. Retrospectively registered.
Keywords: M-charts; Metamorphopsia; Microperimetry; Rhegmatogenous retinal detachment.
Conflict of interest statement
The authors declare that they have no competing interests.
Katarzyna Nowomiejska declares that she is a member of the editorial board of this journal.
Figures
References
-
- Neffendorf JE, Gupta B, Williamson TH. The role of intraocular gas tamponade in rhegmatogenous retinal detachment. Retina. 2017;26. - PubMed
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
