

Risk factors for diagnostic delay in idiopathic pulmonary fibrosis
- PMID: 31126287
- PMCID: PMC6534848
- DOI: 10.1186/s12931-019-1076-0
Risk factors for diagnostic delay in idiopathic pulmonary fibrosis
Abstract
Background: Surveys and retrospective studies of patients with idiopathic pulmonary fibrosis (IPF) have shown a significant diagnostic delay. However, the causes and risk factors for this delay are not known.
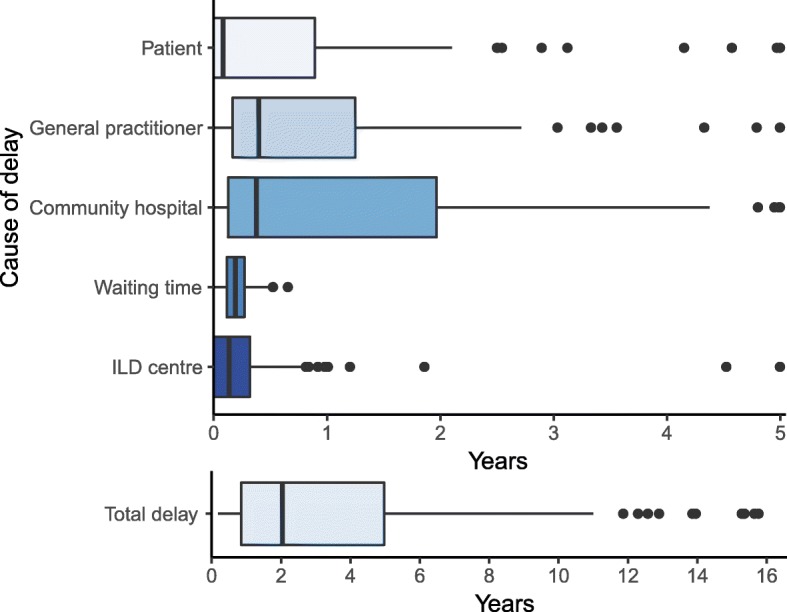
Methods: Dates at six time points before the IPF diagnosis (onset of symptoms, first contact to a general practitioner, first hospital contact, referral to an interstitial lung disease (ILD) centre, first visit at an ILD centre, and final diagnosis) were recorded in a multicentre cohort of 204 incident IPF patients. Based on these dates, the delay was divided into specific patient-related and healthcare-related delays. Demographic and clinical data were used to determine risk factors for a prolonged delay, using multivariate negative binomial regression analysis.
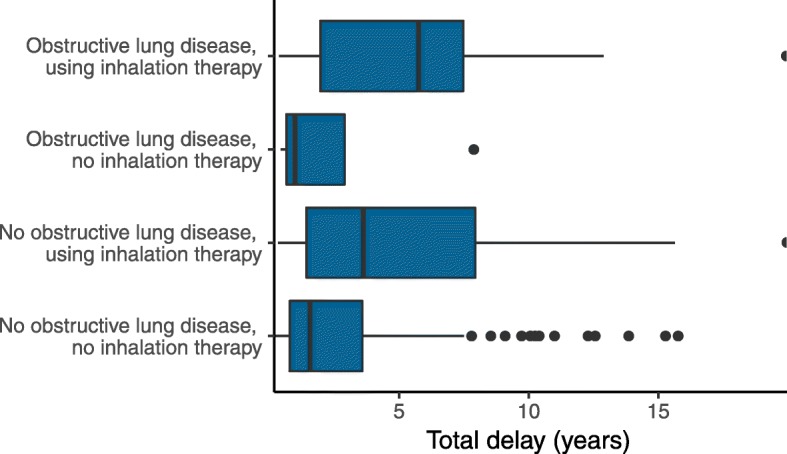
Results: The median diagnostic delay was 2.1 years (IQR: 0.9-5.0), mainly attributable to the patients, general practitioners and community hospitals. Male sex was a risk factor for patient delay (IRR: 3.84, 95% CI: 1.17-11.36, p = 0.006) and old age was a risk factor for healthcare delay (IRR: 1.03, 95% CI: 1.01-1.06, p = 0.004). The total delay was prolonged in previous users of inhalation therapy (IRR: 1.99, 95% CI: 1.40-2.88, p < 0.0001) but not in patients with airway obstruction. Misdiagnosis of respiratory symptoms was reported by 41% of all patients.
Conclusion: Despite increased awareness of IPF, the diagnostic delay is still 2.1 years. Male sex, older age and treatment attempts for alternative diagnoses are risk factors for a delayed diagnosis of IPF. Efforts to reduce the diagnostic delay should focus on these risk factors.
Trial registration: This study was registered at http://clinicaltrials.gov (NCT02772549) on May 10, 2016.
Keywords: Cohort; Delay; Diagnosis; IPF; Observational.
Conflict of interest statement
Dr. Hoyer reports grants from P.A. Messerschmidt og Hustrus Fond, grants from Skibsreder Per Henriksen, R. og Hustrus Fond and grants from Roche a/s, during the conduct of the study. Dr. Skovhus Prior reports lecture fees from Roche A/S and Boehringer Ingelheim Denmark. Dr. Bendstrup reports grants, personal fees and other from Roche, grants, personal fees and other from Boehringer Ingelheim, outside the submitted work. Dr. Wilcke has nothing to disclose. Dr. Shaker reports lecture fees and travel expenses for participation in scientific meetings and congresses from Roche, Boehringer Ingelheim and AstraZeneca and payment for advisory board meetings arranged by Roche and Boehringer Ingelheim.
Figures

References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
