

Results from a Phase IIb, Randomized, Multicenter Study of GVAX Pancreas and CRS-207 Compared with Chemotherapy in Adults with Previously Treated Metastatic Pancreatic Adenocarcinoma (ECLIPSE Study)
- PMID: 31126960
- PMCID: PMC7376746
- DOI: 10.1158/1078-0432.CCR-18-2992
Results from a Phase IIb, Randomized, Multicenter Study of GVAX Pancreas and CRS-207 Compared with Chemotherapy in Adults with Previously Treated Metastatic Pancreatic Adenocarcinoma (ECLIPSE Study)
Abstract
Purpose: Limited options exist for patients with advanced pancreatic cancer progressing after 1 or more lines of therapy. A phase II study in patients with previously treated metastatic pancreatic cancer showed that combining GVAX pancreas (granulocyte-macrophage colony-stimulating factor-secreting allogeneic pancreatic tumor cells) with cyclophosphamide (Cy) and CRS-207 (live, attenuated Listeria monocytogenes expressing mesothelin) resulted in median overall survival (OS) of 6.1 months, which compares favorably with historical OS achieved with chemotherapy. In the current study, we compared Cy/GVAX + CRS-207, CRS-207 alone, and standard chemotherapy in a three-arm, randomized, controlled phase IIb trial.
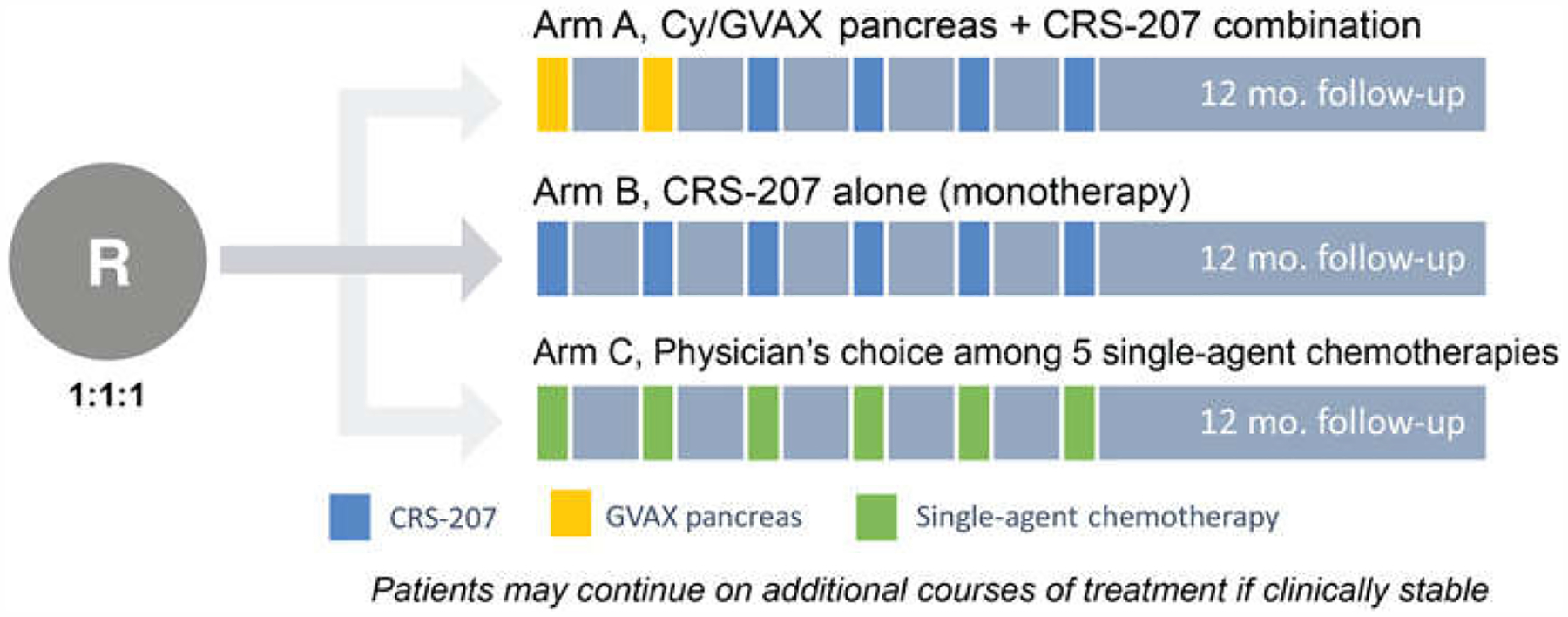
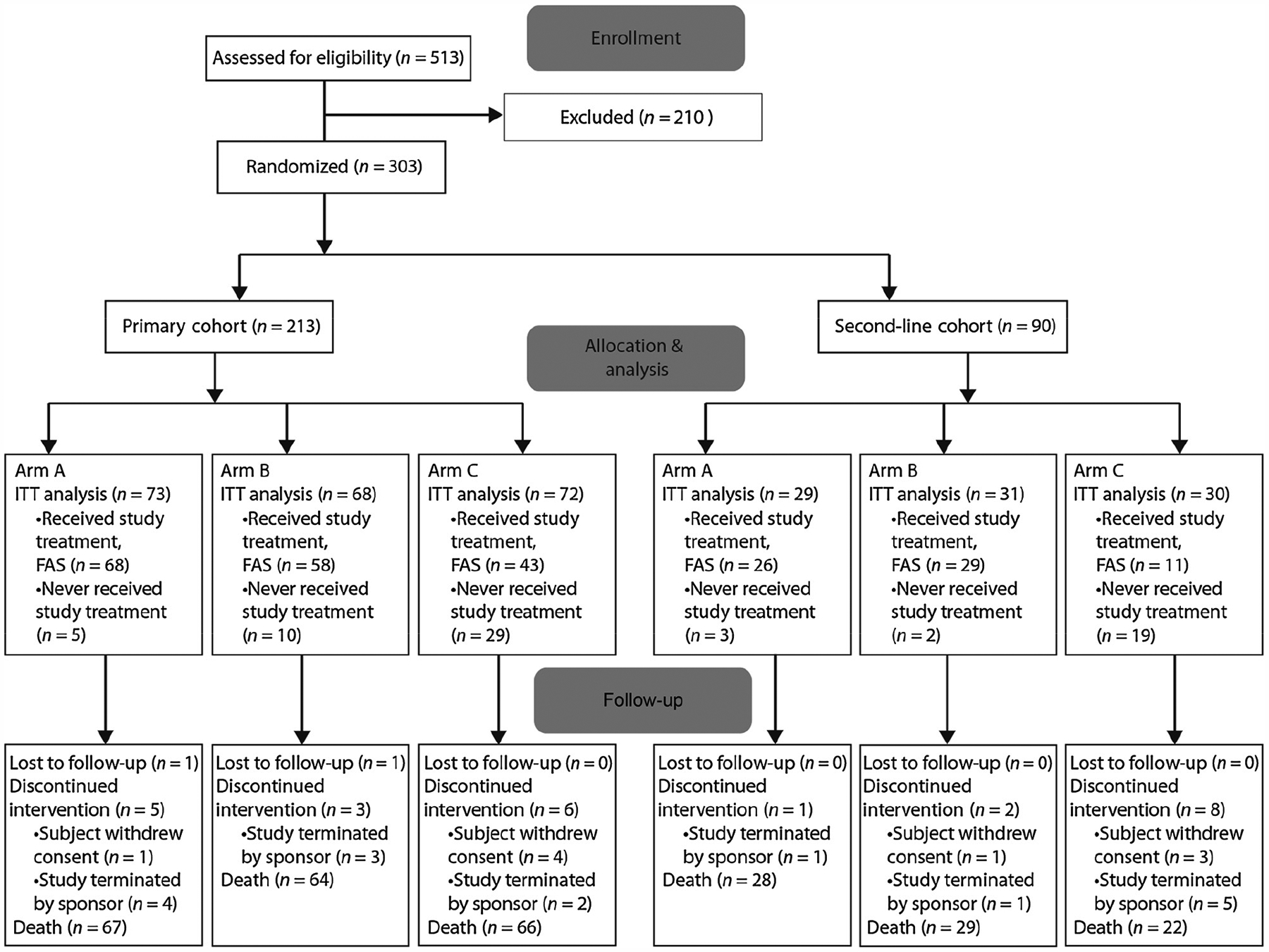
Patients and methods: Patients with previously treated metastatic pancreatic adenocarcinoma were randomized 1:1:1 to receive Cy/GVAX + CRS-207 (arm A), CRS-207 (arm B), or physician's choice of single-agent chemotherapy (arm C). The primary cohort included patients who had failed ≥2 prior lines of therapy, including gemcitabine. The primary objective compared OS between arms A and C in the primary cohort. The second-line cohort included patients who had received 1 prior line of therapy. Additional objectives included OS between all treatment arms, safety, and tumor responses.
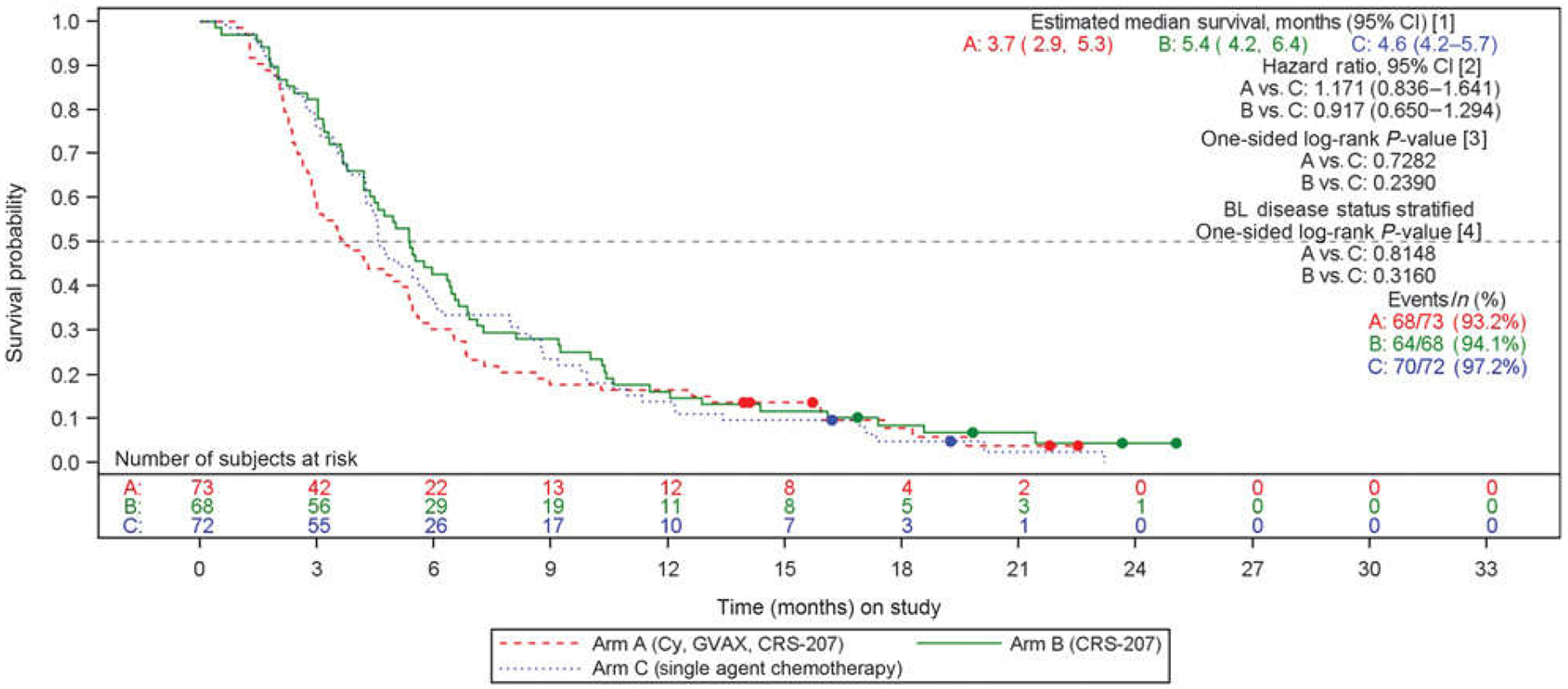
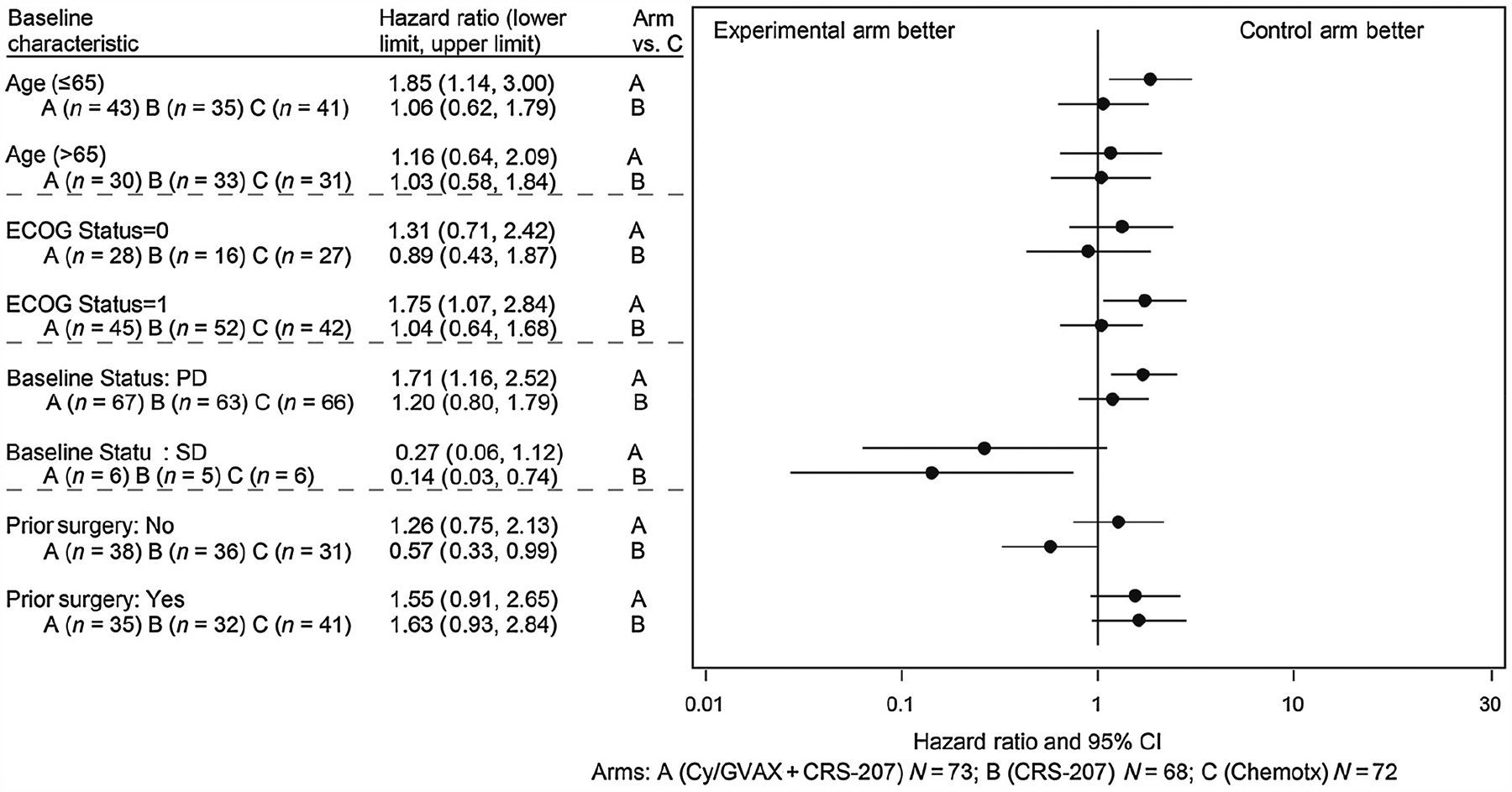
Results: The study did not meet its primary efficacy endpoint. At the final study analysis, median OS [95% confidence interval (CI)] in the primary cohort (N = 213) was 3.7 (2.9-5.3), 5.4 (4.2-6.4), and 4.6 (4.2-5.7) months in arms A, B, and C, respectively, showing no significant difference between arm A and arm C [P = not significant (NS), HR = 1.17; 95% CI, 0.84-1.64]. The most frequently reported adverse events in all treatment groups were chills, pyrexia, fatigue, and nausea. No treatment-related deaths occurred.
Conclusions: The combination of Cy/GVAX + CRS-207 did not improve survival over chemotherapy. (ClinicalTrials.gov ID: NCT02004262)See related commentary by Salas-Benito et al., p. 5435.
©2019 American Association for Cancer Research.
Conflict of interest statement
Disclosure of Potential Conflicts of Interest
D.T. Le reports receiving commercial research grants from Aduro Biotech. A.H. Ko reports receiving commercial research grants to his institution from Celgene, Halozyme, Roche/Genentech, and Aduro Biotech, and is a consultant/advisory board member for Erytech, Celgene, and ARMO Biosciences. Z.A. Wainberg is a consultant/advisory board member for Merck, Five Prime Therapeutics, Novartis, and Lilly. H. Kindler is a consultant/advisory board member for AstraZeneca, Merck, Aldeyra Therapeutics, Astellas, Boehinger Ingelheim, Bristol-Myers Squibb, Erytech, Five Prime Therapeutics, Ipsen, Kyowa, and Paredox Therapeutics. A. Wang-Gillam is a consultant/advisory board member for Tyme, Merrimack, Ipsen, Bristol-Myers Squibb, Pfizer, Jacobio, and Newlink. P. Oberstein reports receiving commercial research grants from Merck; reports receiving other commercial research support from Halozyme, Genentech, Incyte, and AstraZeneca; and is a consultant/advisory board member for Merck, Purdue Pharma, Celgene, Eisai, OncLive, Tyme, Ipsen, Pfizer, Haolzyme, and Angiodynamics. H.J. Zeh III reports receiving commercial research grants from Merck Sharp & Dohme and speakers bureau honoraria from Intuitive Surgical. E. Borazanci reports receiving speakers bureau honoraria from Ipsen, Taiho, Biogen, Genzyme, Novartis, Teva, and Genentech, and is a consultant/advisory board member for Corcept, Ipsen, and Fujifilm. T. Crocenzi reports receiving other commercial research support from Bristol-Myers Squibb and AstraZeneca. A. Murphy holds ownership interest (including patents) in Aduro Biotech. A. Enstrom is an employee of Tempest Therapeutics and Amplion. D.G. Brockstedt is an employee of and holds ownership interest (including patents) in Aduro Biotech. E.M. Jaffee is an employee of Lustgarten Foundation; reports receiving commercial research grants from Aduro Biotech and Bristol-Myers Squibb; reports receiving other commercial research support from Amgen and Hertig; holds ownership interest (including patents) in Aduro Biotech; and is a consultant/advisory board member for CSTONE, DragonFly, and Genocea. No potential conflicts of interest were disclosed by the other authors.
Figures
Comment in
-
Vaccination for Pancreatic Ductal Adenocarcinoma: A Hard Nut to Crack.Clin Cancer Res. 2019 Sep 15;25(18):5435-5437. doi: 10.1158/1078-0432.CCR-19-1753. Epub 2019 Jul 17. Clin Cancer Res. 2019. PMID: 31315885
Comment on
-
Vaccination for Pancreatic Ductal Adenocarcinoma: A Hard Nut to Crack.Clin Cancer Res. 2019 Sep 15;25(18):5435-5437. doi: 10.1158/1078-0432.CCR-19-1753. Epub 2019 Jul 17. Clin Cancer Res. 2019. PMID: 31315885
References
-
- Pancreatic Cancer Treatment (PDQ)-Health Professional Version; [about 4 screens]. [cited 2018 Mar 6]. National Cancer Institute; Available from: https://www.cancer.gov/types/pancreatic/hp/pancreatic-treatment-pdq.
-
- Pancreatic cancer. Oklahoma City (OK): American Cancer Society; 2014. Available from: http://www.cancer.org/acs/groups/cid/documents/webcontent/003131-pdf.pdf.
-
- Wang-Gillam A, Li CP, Bodoky G, Dean A, Shan YS, Jameson G, et al. Nanoliposomal irinotecan with fluorouracil and folinic acid in metastatic pancreatic cancer after previous gemcitabine-based therapy (NAPOLI-1): a global, randomised, open-label, phase 3 trial. Lancet 2016;387:545–57. - PubMed
-
- Santoni M, Battelli N, Buti S. Durvalumab in stage III non-small-cell lung cancer. N Engl J Med 2018;378:869. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
