

Smoking, Alcohol, and Biliary Tract Cancer Risk: A Pooling Project of 26 Prospective Studies
- PMID: 31127946
- PMCID: PMC6910180
- DOI: 10.1093/jnci/djz103
Smoking, Alcohol, and Biliary Tract Cancer Risk: A Pooling Project of 26 Prospective Studies
Abstract
Background: Tobacco and alcohol are well-established risk factors for numerous cancers, yet their relationship to biliary tract cancers remains unclear.
Methods: We pooled data from 26 prospective studies to evaluate associations of cigarette smoking and alcohol consumption with biliary tract cancer risk. Study-specific hazard ratios (HRs) and 95% confidence intervals (CIs) for associations with smoking and alcohol consumption were calculated. Random-effects meta-analysis produced summary estimates. All statistical tests were two-sided.
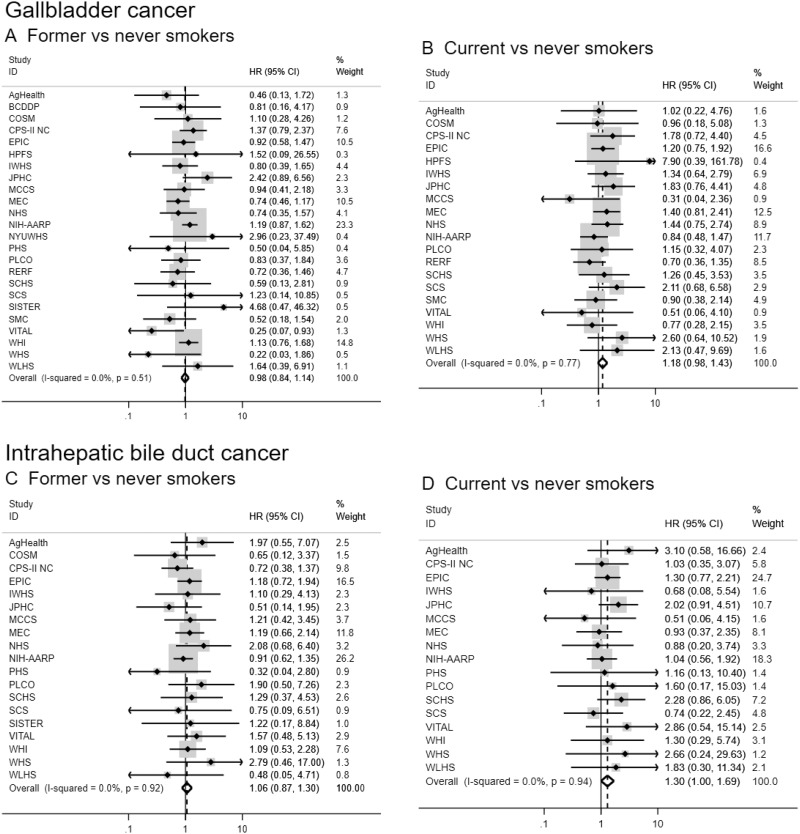
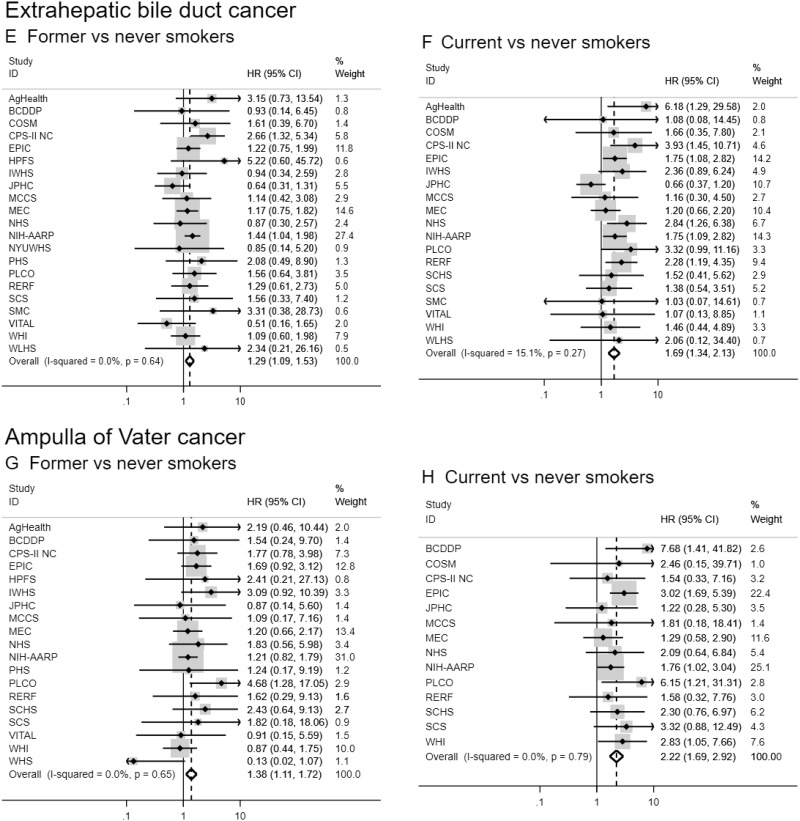
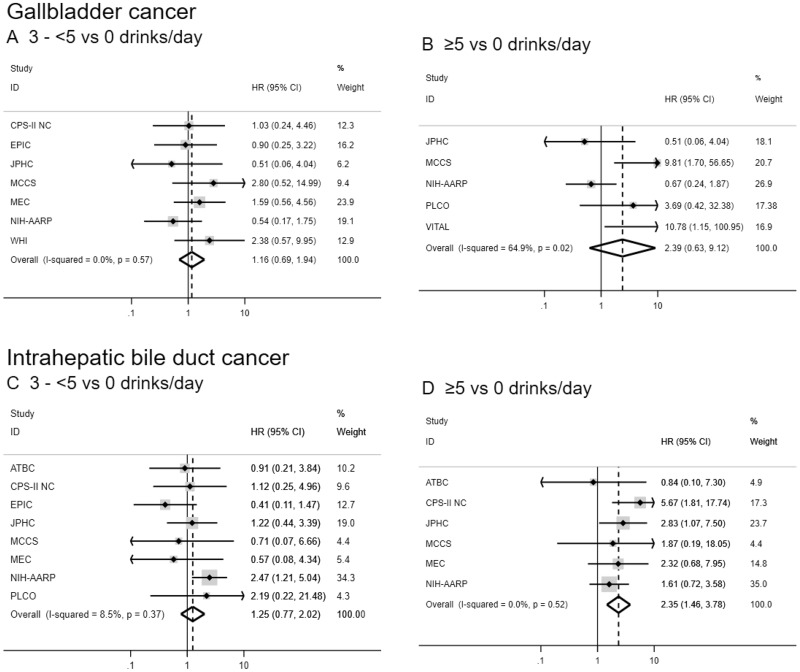
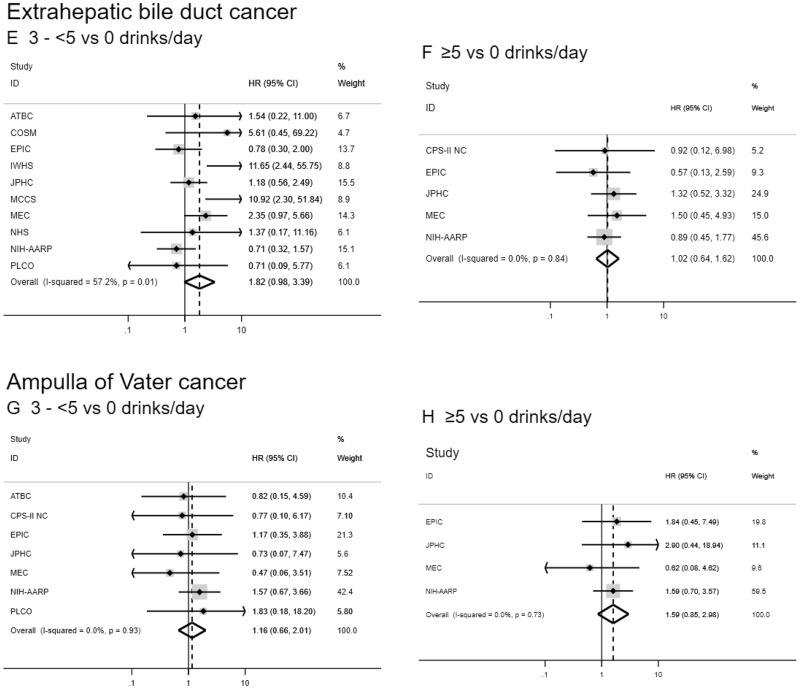
Results: Over a period of 38 369 156 person-years of follow-up, 1391 gallbladder, 758 intrahepatic bile duct, 1208 extrahepatic bile duct, and 623 ampulla of Vater cancer cases were identified. Ever, former, and current smoking were associated with increased extrahepatic bile duct and ampulla of Vater cancers risk (eg, current vs never smokers HR = 1.69, 95% CI = 1.34 to 2.13 and 2.22, 95% CI = 1.69 to 2.92, respectively), with dose-response effects for smoking pack-years, duration, and intensity (all Ptrend < .01). Current smoking and smoking intensity were also associated with intrahepatic bile duct cancer (eg, >40 cigarettes per day vs never smokers HR = 2.15, 95 % CI = 1.15 to 4.00; Ptrend = .001). No convincing association was observed between smoking and gallbladder cancer. Alcohol consumption was only associated with intrahepatic bile duct cancer, with increased risk for individuals consuming five or more vs zero drinks per day (HR = 2.35, 95%CI = 1.46 to 3.78; Ptrend = .04). There was evidence of statistical heterogeneity among several cancer sites, particularly between gallbladder cancer and the other biliary tract cancers.
Conclusions: Smoking appears to increase the risk of developing all biliary tract cancers except gallbladder cancer. Alcohol may increase the risk of intrahepatic bile duct cancer. Findings highlight etiologic heterogeneity across the biliary tract.
Published by Oxford University Press 2019. This work is written by US Government employees and is in the public domain in the United States.
Figures
References
-
- Hsing A, Rashid A, Devesa S, et al. Biliary tract cancer In: Schottenfeld D, Fraumeni JF Jr eds. Cancer Epidemiology and Prevention. 3rd ed. New York: Oxford University Press, Inc; 2006:787–800.
-
- Njei B. Changing pattern of epidemiology in intrahepatic cholangiocarcinoma. Hepatology. 2014;60(3):1107–1108. - PubMed
-
- Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136(5):E359–E386. - PubMed
-
- Patel T. Increasing incidence and mortality of primary intrahepatic cholangiocarcinoma in the United States. Hepatology. 2001;33(6):1353–1357. - PubMed
Publication types
MeSH terms
Grants and funding
- HHSN268201600001C/HL/NHLBI NIH HHS/United States
- HHSN268201600003C/HL/NHLBI NIH HHS/United States
- UM1 CA182876/CA/NCI NIH HHS/United States
- U01 CA152939/CA/NCI NIH HHS/United States
- BHF_/British Heart Foundation/United Kingdom
- U01 CA182934/CA/NCI NIH HHS/United States
- R01 CA043092/CA/NCI NIH HHS/United States
- Z01 ES049030/ImNIH/Intramural NIH HHS/United States
- K05 CA154337/CA/NCI NIH HHS/United States
- HHSN261201500005C/CA/NCI NIH HHS/United States
- HHSN268201600002C/HL/NHLBI NIH HHS/United States
- R01 CA080205/CA/NCI NIH HHS/United States
- HHSN268201600018C/HL/NHLBI NIH HHS/United States
- R01 CA144034/CA/NCI NIH HHS/United States
- P30 ES000260/ES/NIEHS NIH HHS/United States
- WT_/Wellcome Trust/United Kingdom
- DH_/Department of Health/United Kingdom
- UM1 CA182934/CA/NCI NIH HHS/United States
- U01 CA164973/CA/NCI NIH HHS/United States
- MRC_/Medical Research Council/United Kingdom
- HHSN268201600004C/HL/NHLBI NIH HHS/United States
- UM1 CA167552/CA/NCI NIH HHS/United States
- UM1 CA186107/CA/NCI NIH HHS/United States
- U01 CA182913/CA/NCI NIH HHS/United States
- Z01 ES044005/ImNIH/Intramural NIH HHS/United States
- CRUK_/Cancer Research UK/United Kingdom
LinkOut - more resources
Full Text Sources
Medical
