

National patterns of care and fertility outcomes for reproductive-aged women with endometrial cancer or atypical hyperplasia
- PMID: 31128110
- PMCID: PMC7069241
- DOI: 10.1016/j.ajog.2019.05.029
National patterns of care and fertility outcomes for reproductive-aged women with endometrial cancer or atypical hyperplasia
Abstract
Background: Although it is uncommon, the incidence of endometrial cancer and atypical hyperplasia among reproductive-aged women is increasing. The fertility outcomes in this population are not well described.
Objective: We aim to describe the patterns of care and fertility outcomes of reproductive-aged women with endometrial cancer or atypical hyperplasia.
Materials and methods: A cohort of women aged ≤45 years with endometrial cancer or atypical hyperplasia diagnosed in 2000 to 2014 were identified in Truven Marketscan, an insurance claims database of commercially insured patients in the United States. Treatment information, including use of progestin therapy, hysterectomy, and assisted fertility services, was identified and collected using a combination of Common Procedural Terminology codes, International Statistical Classification of Diseases and Related Health Problems codes, and National Drug Codes. Pregnancy events were identified from claims data using a similar technique. Patients were categorized as receiving progestin therapy alone, progestin therapy followed by hysterectomy, or standard surgical management with hysterectomy alone. Multivariable logistic regression was performed to assess factors associated with receiving fertility-sparing treatment.
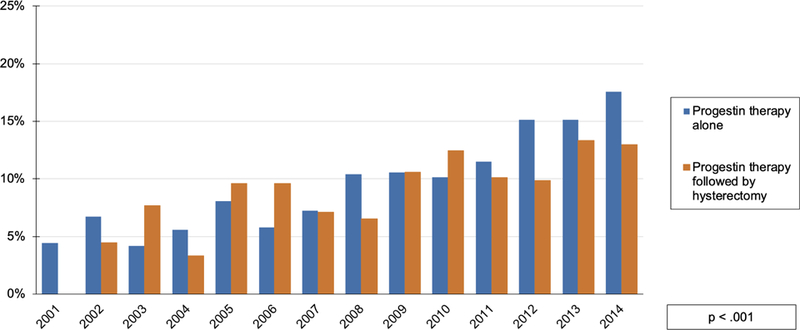
Results: A total of 4007 reproductive-aged patients diagnosed with endometrial cancer or atypical hyperplasia were identified. The majority of these patients (n = 3189; 79.6%) received standard surgical management. Of the 818 patients treated initially with progestins, 397 (48.5%) subsequently underwent hysterectomy, whereas 421 (51.5%) did not. Patients treated with progestin therapy had a lower median age than those who received standard surgical management (median age, 36 vs 41 years; P < .001). The proportion of patients receiving progestin therapy increased significantly over the observation period, with 24.9% treated at least initially with progestin therapy in 2014 (P < .001). Multivariable analysis shows that younger age, a diagnosis of atypical hyperplasia diagnosis rather than endometrial cancer, and diagnosis later in the study period were all associated with a greater likelihood of receiving progestin therapy (P < .0001). Among the 421 patients who received progestin therapy alone, 92 patients (21.8%; 92/421) had 131 pregnancies, including 49 live births for a live birth rate of 11.6%. Among the 397 patients treated with progestin therapy followed by hysterectomy, 25 patients (6.3%; 25/397) had 34 pregnancies with 13 live births. The median age of patients who experienced a live birth following diagnosis during the study period was 36 years (interquartile range, 33-38). The use of some form of assisted fertility services was observed in 15.5% patients who were treated with progestin therapy. Among patients who experienced any pregnancy event following diagnosis, 54% of patients used some form of fertility treatment. For patients who experienced a live birth following diagnosis, 50% of patients received fertility treatment. Median time to live birth following diagnosis was 756 days (interquartile range, 525-1077). Patients treated with progestin therapy were more likely to experience a live birth if they had used assisted fertility services (odds ratio, 5.9; 95% confidence interval, 3.4-10.1; P < .0001).
Conclusion: The number of patients who received fertility-sparing treatment for endometrial cancer or atypical hyperplasia increased over time. However, the proportion of women who experience a live birth following these diagnoses is relatively small.
Keywords: endometrial cancer; endometrial hyperplasia; fertility; fertility conservation; fertility-sparing treatment; health services research; oncofertility.
Copyright © 2019 Elsevier Inc. All rights reserved.
Figures

Similar articles
-
Chances of pregnancy and live birth among women undergoing conservative management of early-stage endometrial cancer: a systematic review and meta-analysis.Hum Reprod Update. 2022 Feb 28;28(2):282-295. doi: 10.1093/humupd/dmab041. Hum Reprod Update. 2022. PMID: 34935045 Free PMC article.
-
Fertility sparing treatment of complex atypical hyperplasia and low grade endometrial cancer using oral progestin.Gynecol Oncol. 2014 May;133(2):229-33. doi: 10.1016/j.ygyno.2014.02.020. Epub 2014 Feb 19. Gynecol Oncol. 2014. PMID: 24561246
-
[Pregnant rate and pregnancy-relating factors of patients with early endometrial carcinoma and severe atypical hyperplasia of endometrium after fertility-preserving treatment by progestin].Zhonghua Fu Chan Ke Za Zhi. 2013 Jul;48(7):519-22. Zhonghua Fu Chan Ke Za Zhi. 2013. PMID: 24284224 Chinese.
-
Prognostic factors of oncological and reproductive outcomes in fertility-sparing treatment of complex atypical hyperplasia and low-grade endometrial cancer using oral progestin in Chinese patients.Gynecol Oncol. 2015 Dec;139(3):424-8. doi: 10.1016/j.ygyno.2015.09.078. Epub 2015 Sep 30. Gynecol Oncol. 2015. PMID: 26428941
-
Outcomes of women treated with progestin and metformin for atypical endometrial hyperplasia and early endometrial cancer: a systematic review and meta-analysis.Int J Gynecol Cancer. 2021 Dec;31(12):1499-1505. doi: 10.1136/ijgc-2021-002699. Epub 2021 Nov 16. Int J Gynecol Cancer. 2021. PMID: 34785524
Cited by
-
Stromal Pbrm1 mediates chromatin remodeling necessary for embryo implantation in the mouse uterus.J Clin Invest. 2024 Mar 1;134(5):e174194. doi: 10.1172/JCI174194. J Clin Invest. 2024. PMID: 38426493 Free PMC article.
-
Conservative management of early-stage endometrial cancer for fertility preservation: a survey study among Swedish gynecologists and gynecological oncologists.Sci Rep. 2023 Apr 11;13(1):5861. doi: 10.1038/s41598-023-32911-y. Sci Rep. 2023. PMID: 37041242 Free PMC article.
-
Fertility-Sparing Surgery in Gynecologic Cancer: A Systematic Review.Cancers (Basel). 2021 Feb 28;13(5):1008. doi: 10.3390/cancers13051008. Cancers (Basel). 2021. PMID: 33670929 Free PMC article. Review.
-
Fertility-Sparing Treatment for Early-Stage Cervical, Ovarian, and Endometrial Malignancies.Obstet Gynecol. 2020 Dec;136(6):1157-1169. doi: 10.1097/AOG.0000000000004163. Obstet Gynecol. 2020. PMID: 33156194 Free PMC article. Review.
-
Chances of pregnancy and live birth among women undergoing conservative management of early-stage endometrial cancer: a systematic review and meta-analysis.Hum Reprod Update. 2022 Feb 28;28(2):282-295. doi: 10.1093/humupd/dmab041. Hum Reprod Update. 2022. PMID: 34935045 Free PMC article.
References
-
- Noone AMHN, Krapcho M, Miller D, Brest A, Yu M, Ruhl J, Tatalovich Z, Mariotto A, Lewis DR, Chen HS, Feuer EJ, Cronin KA. SEER Cancer Statistics Review, 1975–2015 Bethesda, MD: National Cancer Institute; April 2018 2018.
-
- Group SGOCPECW, Burke WM, Orr J, et al. Endometrial cancer: a review and current management strategies: part II. Gynecol Oncol 2014;134(2):393–402. - PubMed
-
- Group SGOCPECW, Burke WM, Orr J, et al. Endometrial cancer: a review and current management strategies: part I. Gynecol Oncol 2014;134(2):385–392. - PubMed
-
- Rodolakis A, Biliatis I, Morice P, et al. European Society of Gynecological Oncology Task Force for Fertility Preservation: Clinical Recommendations for Fertility-Sparing Management in Young Endometrial Cancer Patients. Int J Gynecol Cancer 2015;25(7):1258–1265. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
