

A Multidimensional Profile of Dyspnea in Hospitalized Patients
- PMID: 31128117
- PMCID: PMC7090324
- DOI: 10.1016/j.chest.2019.04.128
A Multidimensional Profile of Dyspnea in Hospitalized Patients
Abstract
Background: Dyspnea is prevalent among hospitalized patients but little is known about the experience of dyspnea among inpatients. We sought to characterize the multiple sensations and associated emotions of dyspnea in patients admitted with dyspnea to a tertiary care hospital.
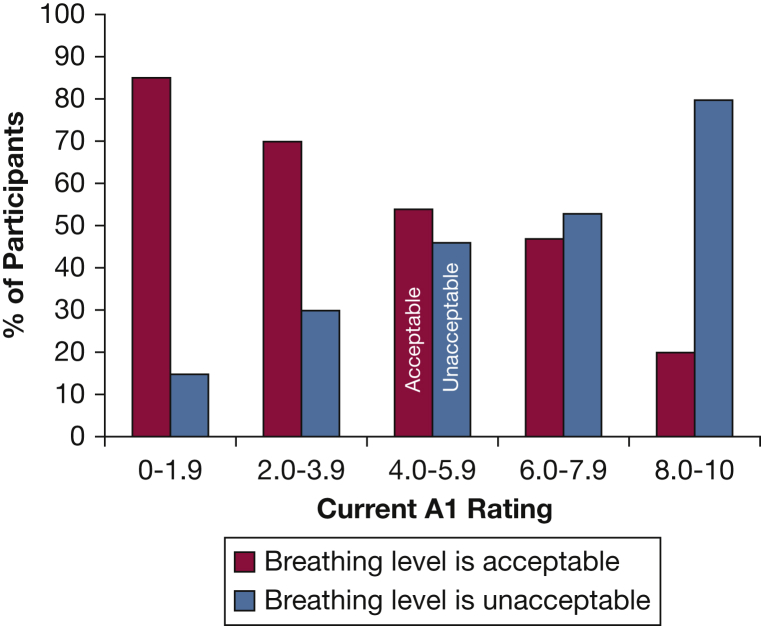
Methods: We selected patients who reported breathing discomfort of at least 4/10 on admission (10 = unbearable). Research staff recruited 156 patients within 24 hours of admission and evaluated daily patients' current and worst dyspnea with the Multidimensional Dyspnea Profile; patients participated in the study 2.6 days on average. The Multidimensional Dyspnea Profile assesses overall breathing discomfort (A1), intensity of five sensory qualities of dyspnea, and 5 negative emotional responses to dyspnea. Patients were also asked to rate whether current levels of dyspnea were "acceptable."
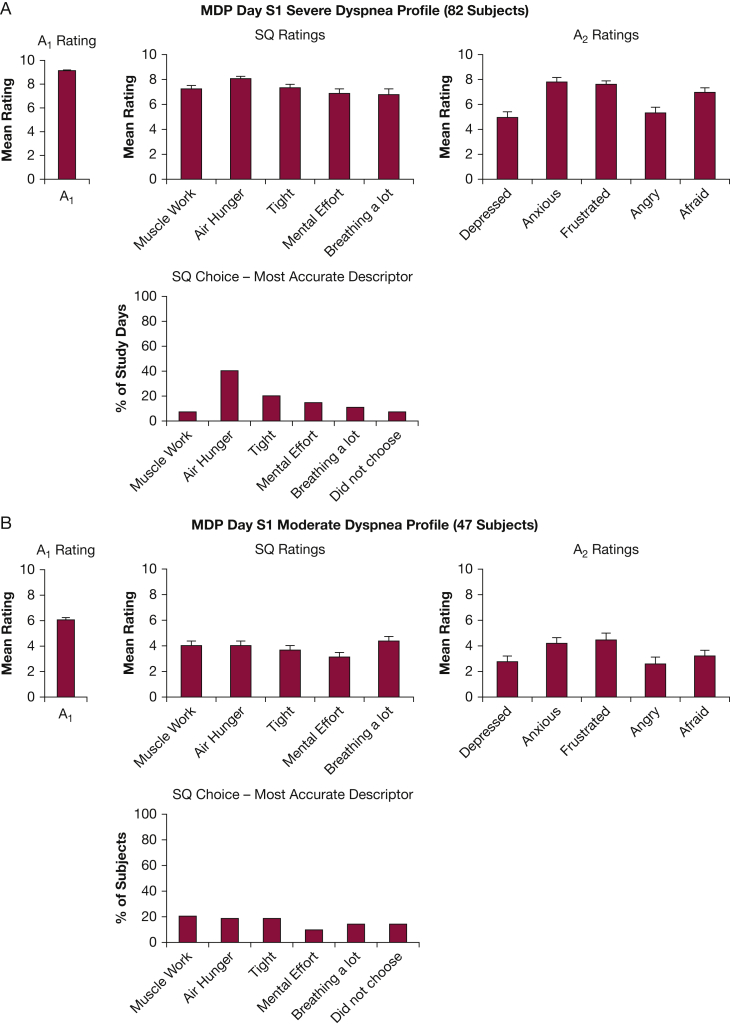
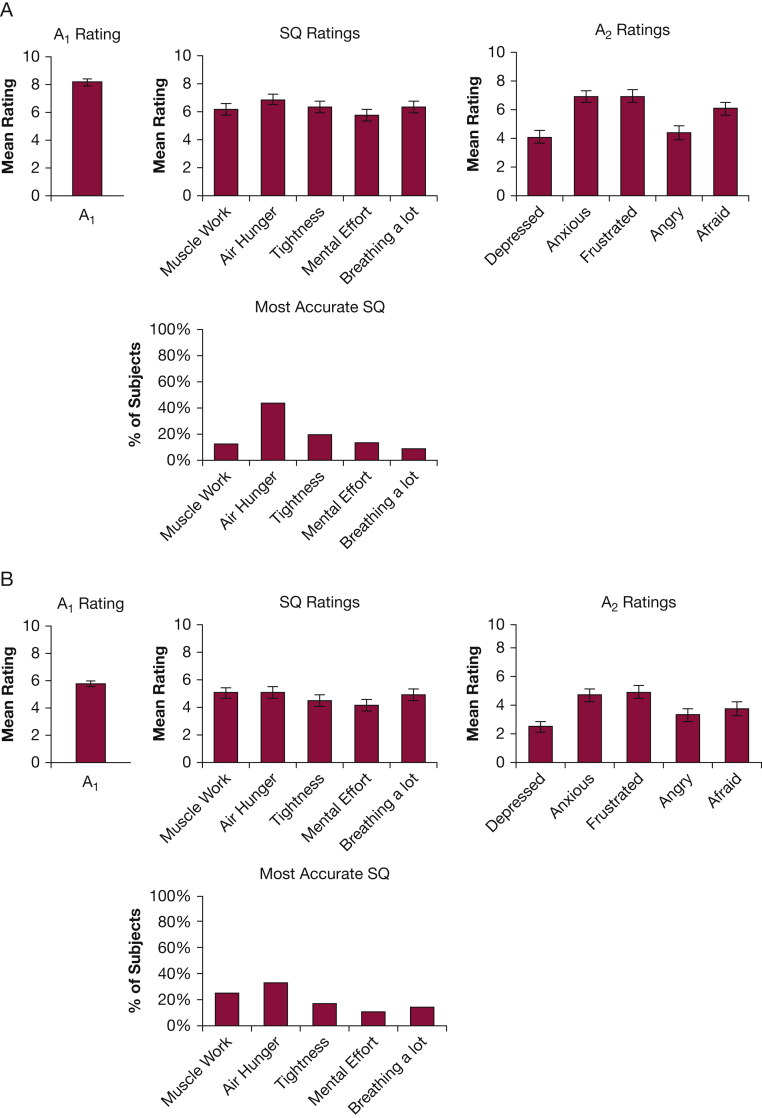
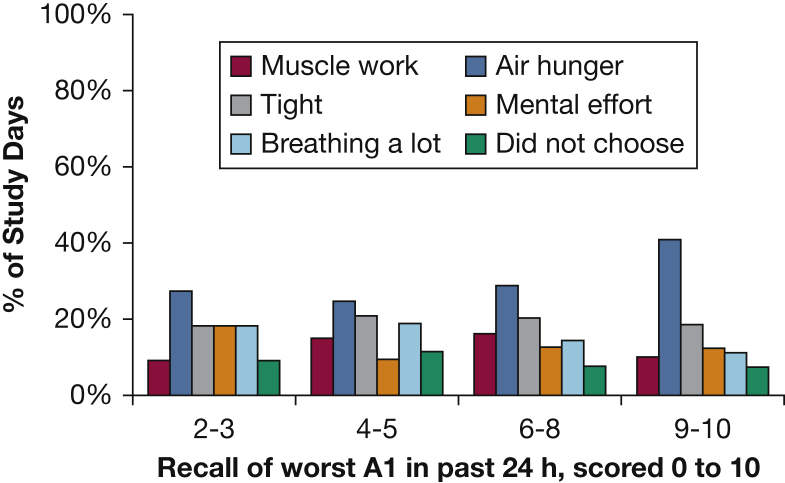
Results: At the time of the first research interview, patients reported slight to moderate dyspnea (A1 median 4); however, most patients reported experiencing severe dyspnea in the 24 hours before the interview (A1 mean 7.8). A total of 54% of patients with dyspnea ≥4 on day 1 found the symptom unacceptable. The worst dyspnea each day in the prior 24 hours usually occurred at rest. Dyspnea declined but persisted through hospitalization for most patients. "Air hunger" was the dominant sensation, especially when dyspnea was strong (>4). Anxiety and frustration were the dominant emotions associated with dyspnea.
Conclusions: This first multidimensional portrait of dyspnea in a general inpatient population characterizes the sensations and emotions dyspneic patients endure. The finding that air hunger is the dominant sensation of severe dyspnea has implications for design of laboratory models of these sensations and may have implications for targets of palliation of symptoms.
Keywords: dyspnea; hospitalized patients; inpatients; symptoms.
Copyright © 2019 American College of Chest Physicians. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Dyspnea affective response: comparing COPD patients with healthy volunteers and laboratory model with activities of daily living.BMC Pulm Med. 2013 Apr 27;13:27. doi: 10.1186/1471-2466-13-27. BMC Pulm Med. 2013. PMID: 23621986 Free PMC article.
-
Multidimensional Dyspnea Profile: an instrument for clinical and laboratory research.Eur Respir J. 2015 Jun;45(6):1681-91. doi: 10.1183/09031936.00038914. Epub 2015 Mar 18. Eur Respir J. 2015. PMID: 25792641 Free PMC article. Review.
-
The affective dimension of laboratory dyspnea: air hunger is more unpleasant than work/effort.Am J Respir Crit Care Med. 2008 Jun 15;177(12):1384-90. doi: 10.1164/rccm.200711-1675OC. Epub 2008 Mar 27. Am J Respir Crit Care Med. 2008. PMID: 18369200 Free PMC article. Clinical Trial.
-
Prevalence of Dyspnea Among Hospitalized Patients at the Time of Admission.J Pain Symptom Manage. 2018 Jul;56(1):15-22.e2. doi: 10.1016/j.jpainsymman.2018.02.013. Epub 2018 Feb 22. J Pain Symptom Manage. 2018. PMID: 29476798 Free PMC article.
-
Mechanisms underlying the sensation of dyspnea.Respir Investig. 2021 Jan;59(1):66-80. doi: 10.1016/j.resinv.2020.10.007. Epub 2020 Dec 1. Respir Investig. 2021. PMID: 33277231 Review.
Cited by
-
Dyspnea in the ICU: It Is Difficult to See What Patients Feel.Am J Respir Crit Care Med. 2023 Jul 1;208(1):6-7. doi: 10.1164/rccm.202304-0677ED. Am J Respir Crit Care Med. 2023. PMID: 37159946 Free PMC article. No abstract available.
-
Prevalence and severity of differing dimensions of breathlessness among elderly males in the population.ERJ Open Res. 2021 Feb 7;8(1):00553-2021. doi: 10.1183/23120541.00553-2021. eCollection 2022 Jan. ERJ Open Res. 2021. PMID: 35141316 Free PMC article.
-
Management of Refractory Breathlessness: a Review for General Internists.J Gen Intern Med. 2021 Apr;36(4):1035-1040. doi: 10.1007/s11606-020-06439-0. Epub 2021 Jan 19. J Gen Intern Med. 2021. PMID: 33469757 Free PMC article. Review.
-
Danish translation and linguistic validation of the multidimensional dyspnea profile.Eur Clin Respir J. 2021 Mar 30;8(1):1905498. doi: 10.1080/20018525.2021.1905498. Eur Clin Respir J. 2021. PMID: 33854743 Free PMC article. No abstract available.
-
Dyspnea, Acute Respiratory Failure, Psychological Trauma, and Post-ICU Mental Health: A Caution and a Call for Research.Chest. 2021 Feb;159(2):749-756. doi: 10.1016/j.chest.2020.09.251. Epub 2020 Oct 1. Chest. 2021. PMID: 33011205 Free PMC article. Review.
References
-
- Bausewein C., Booth S., Higginson I.J. Measurement of dyspnoea in the clinical rather than the research setting. Curr Opin Support Palliat Care. 2008;2(2):95–99. - PubMed
-
- Dorman S., Byrne A., Edwards A. Which measurement scales should we use to measure breathlessness in palliative care? A systematic review. Palliat Med. 2007;21(3):177–191. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
