

Associations Between Inflammatory Endotypes and Clinical Presentations in Chronic Rhinosinusitis
- PMID: 31128376
- PMCID: PMC6842686
- DOI: 10.1016/j.jaip.2019.05.009
Associations Between Inflammatory Endotypes and Clinical Presentations in Chronic Rhinosinusitis
Abstract
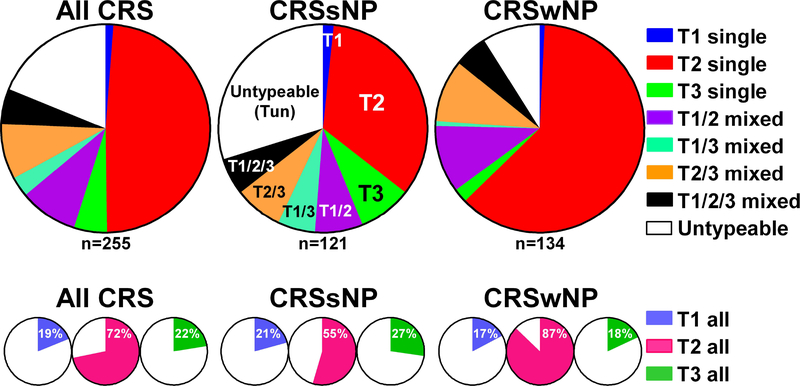
Background: Chronic rhinosinusitis (CRS) is a heterogeneous disease characterized by mucosal inflammation in the nose and paranasal sinuses. Inflammation in CRS is also heterogeneous and is mainly characterized by type 2 (T2) inflammation, but subsets of patients show type 1 (T1) and type 3 (T3) inflammation. Whether inflammatory endotypes are associated with clinical phenotypes has yet to be explored in detail.
Objective: To identify associations between inflammatory endotypes and clinical presentations in CRS.
Methods: We compared 121 patients with nonpolypoid CRS (CRSsNP) and 134 patients with polypoid CRS (CRSwNP) and identified inflammatory endotypes using markers including IFN-γ (T1), eosinophil cationic protein (T2), Charcot-Leyden crystal galectin (T2), and IL-17A (T3). We collected clinical parameters from medical and surgical records and examined whether there were any associations between endotype and clinical features.
Results: The presence of nasal polyps, asthma comorbidity, smell loss, and allergic mucin was significantly associated with the presence of T2 endotype in all patients with CRS. The T1 endotype was significantly more common in females, and the presence of pus was significantly associated with T3 endotype in all patients with CRS. We further analyzed these associations in CRSsNP and CRSwNP separately and found that smell loss was still associated with T2 endotype and pus with the T3 endotype in both CRSsNP and CRSwNP. Importantly, patients with CRS with T2 and T3 mixed endotype tended to have clinical presentations shared by both T2 and T3 endotypes.
Conclusions: Clinical presentations are directly associated with inflammatory endotypes in CRS. Identification of inflammatory endotypes may allow for more precise and personalized medical treatments in CRS.
Keywords: Chronic rhinosinusitis; Clinical presentation; Endotype-phenotype association; Inflammatory endotype.
Copyright © 2019 American Academy of Allergy, Asthma & Immunology. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures



Comment in
-
Endotype-Phenotype Correlation in Chronic Rhinosinusitis: Is It Time to Think Beyond Polyposis?J Allergy Clin Immunol Pract. 2019 Nov-Dec;7(8):2821-2822. doi: 10.1016/j.jaip.2019.07.024. J Allergy Clin Immunol Pract. 2019. PMID: 31706495 No abstract available.
References
-
- Fokkens WJ, Lund VJ, Mullol J, Bachert C, Alobid I, Baroody F, et al. European Position Paper on Rhinosinusitis and Nasal Polyps 2012. Rhinol Suppl 2012; 23:3 p preceding table of contents, 1–298. - PubMed
-
- Orlandi RR, Kingdom TT, Hwang PH, Smith TL, Alt JA, Baroody FM, et al. International Consensus Statement on Allergy and Rhinology: Rhinosinusitis. Int Forum Allergy Rhinol 2016; 6 Suppl 1:S22–209. - PubMed
-
- Smith KA, Orlandi RR, Rudmik L. Cost of adult chronic rhinosinusitis: A systematic review. Laryngoscope 2015; 125:1547–56. - PubMed
-
- Rudmik L Economics of Chronic Rhinosinusitis. Curr Allergy Asthma Rep 2017; 17:20. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
