

Serum CXCL11 correlates with pulmonary outcomes and disease burden in sarcoidosis
- PMID: 31128616
- PMCID: PMC6594698
- DOI: 10.1016/j.rmed.2019.04.005
Serum CXCL11 correlates with pulmonary outcomes and disease burden in sarcoidosis
Abstract
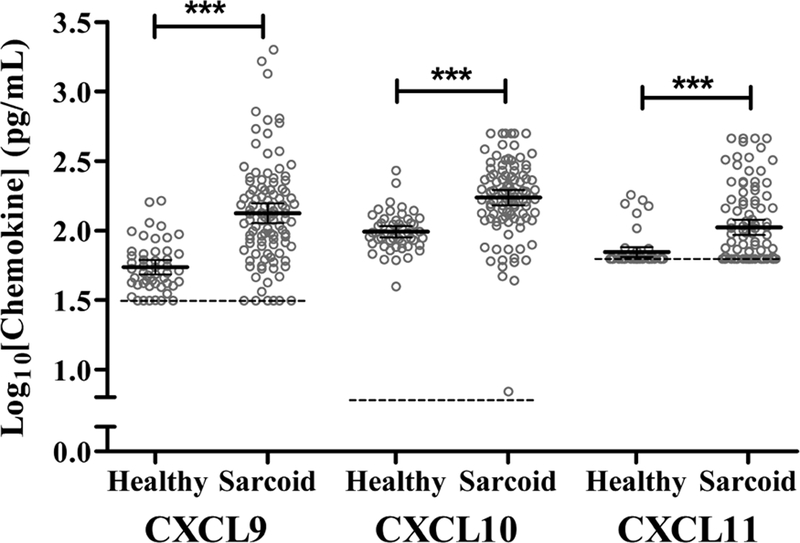
Background: Sarcoidosis is a systemic granulomatous disease of unknown etiology that affects the lungs in 90% of patients, but has a wide range of disease manifestations and outcomes including chronic and progressive courses. Noninvasive biomarkers are needed to assess these outcomes and guide decisions for long term monitoring and treatment. Interferon-gamma (IFN-γ)-inducible chemotactic cytokines (chemokines), CXCL9, CXCL10 and CXCL11, show promise in this regard because they have been implicated in the pathogenesis of and reflect the burden of granulomatous inflammation. CXCL11 has been reported to have unique functional properties in modulating adaptive immunity in model systems so our goal was to examine serum levels of CXCL11 in relation to clinical outcomes in a heterogeneous cohort of sarcoidosis subjects.
Methods: CXCL19, CXCL10, and CXCL11 serum levels were measured in sarcoidosis and healthy subjects using ELISA assay. We determined relationships between CXCL11 and standard clinical inflammatory markers, expression of IFN-γ-related genes in whole blood, organ involvement, dyspnea scores, and measures of pulmonary function.
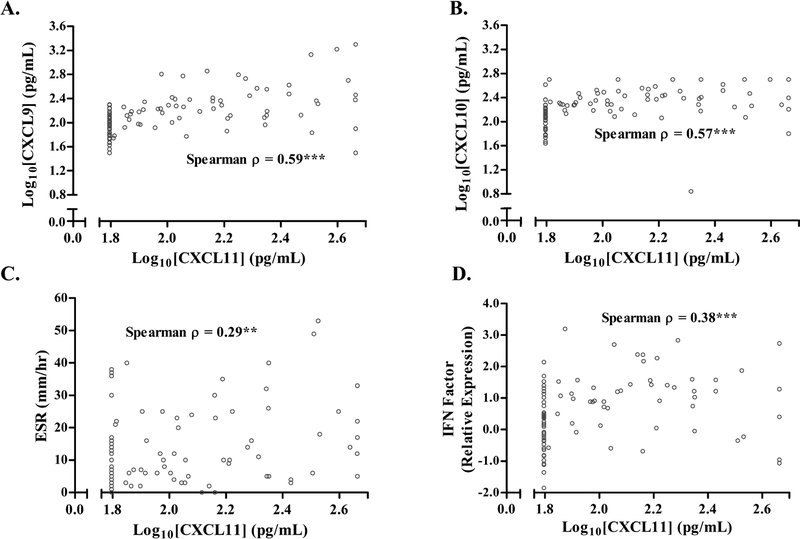
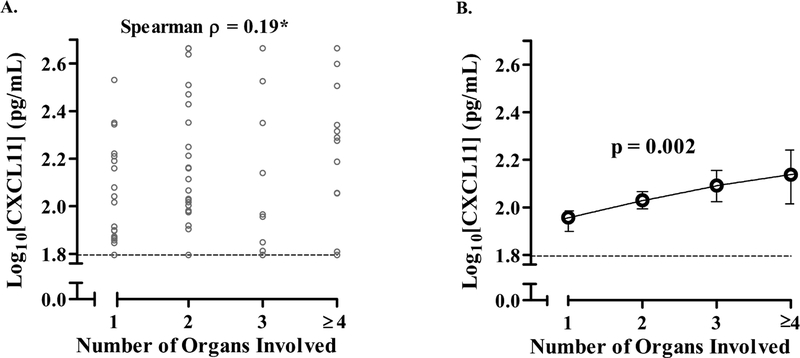
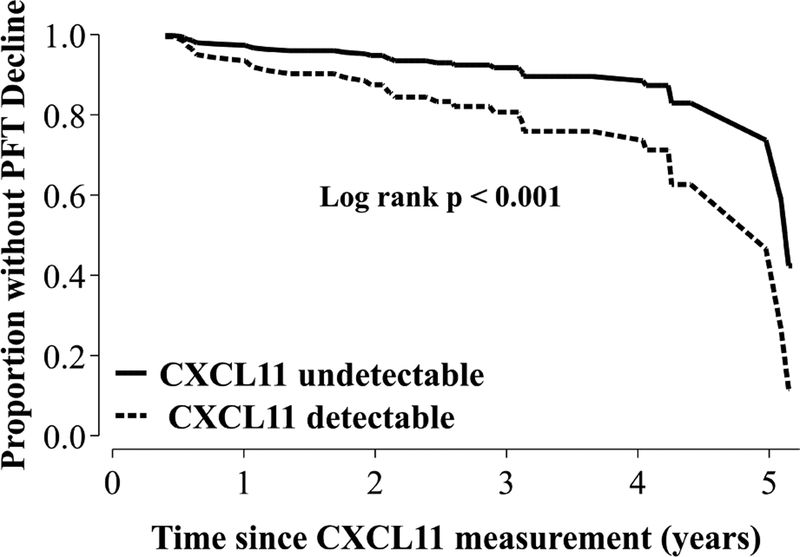
Results: In a cross-sectional analysis of 104 sarcoidosis subjects, serum CXCL11 was significantly elevated compared to 49 healthy controls (p < 0.001). CXCL11 was positively correlated with CXCL9 and CXCL10 (p < 0.001), sedimentation rate (p < 0.01), and mean expression of three IFN-γ-related genes in whole blood (GBP1, STAT1, and STAT2) (p < 0.001). CXCL11 was inversely correlated with FVC %predicted (%pred) and FEV1 %pred and higher levels were associated with higher patient-reported dyspnea scores. We found positive correlations between CXCL11 and number of organs involved. Using survival analyses, we found that CXCL11 levels were predictive of future pulmonary function test (PFT) decline (log rank <0.001 and HR of log10(CXCL11) = 5.1, 95% CI 1.2-21, p = 0.026).
Conclusions: The pattern of expression of serum CXCL11 in sarcoidosis patients suggests that this blood measure could be helpful in identifying patients that need longer-term monitoring for progressive thoracic and extra-thoracic sarcoidosis.
Keywords: CXCL10; CXCL11; CXCL9; Chemokine; Interferon-gamma; Sarcoidosis.
Copyright © 2019 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Figures

References
-
- Chappell AG, Cheung WY, Hutchings HA. Sarcoidosis: a long-term follow up study. Sarcoidosis, vasculitis, and diffuse lung diseases : official journal of WASOG. 2000;17(2):167–73. - PubMed
-
- Inui N, Chida K, Suda T, Nakamura H. TH1/TH2 and TC1/TC2 profiles in peripheral blood and bronchoalveolar lavage fluid cells in pulmonary sarcoidosis. The Journal of allergy and clinical immunology. 2001;107(2):337–44. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
