

Effects of antiplatelet therapy on stroke risk by brain imaging features of intracerebral haemorrhage and cerebral small vessel diseases: subgroup analyses of the RESTART randomised, open-label trial
- PMID: 31129065
- PMCID: PMC7645733
- DOI: 10.1016/S1474-4422(19)30184-X
Effects of antiplatelet therapy on stroke risk by brain imaging features of intracerebral haemorrhage and cerebral small vessel diseases: subgroup analyses of the RESTART randomised, open-label trial
Abstract
Background: Findings from the RESTART trial suggest that starting antiplatelet therapy might reduce the risk of recurrent symptomatic intracerebral haemorrhage compared with avoiding antiplatelet therapy. Brain imaging features of intracerebral haemorrhage and cerebral small vessel diseases (such as cerebral microbleeds) are associated with greater risks of recurrent intracerebral haemorrhage. We did subgroup analyses of the RESTART trial to explore whether these brain imaging features modify the effects of antiplatelet therapy.
Methods: RESTART was a prospective, randomised, open-label, blinded-endpoint, parallel-group trial at 122 hospitals in the UK that assessed whether starting antiplatelet therapy might reduce the risk of recurrent symptomatic intracerebral haemorrhage compared with avoiding antiplatelet therapy. For this prespecified subgroup analysis, consultant neuroradiologists masked to treatment allocation reviewed brain CT or MRI scans performed before randomisation to confirm participant eligibility and rate features of the intracerebral haemorrhage and surrounding brain. We followed participants for primary (recurrent symptomatic intracerebral haemorrhage) and secondary (ischaemic stroke) outcomes for up to 5 years (reported elsewhere). For this report, we analysed eligible participants with intracerebral haemorrhage according to their treatment allocation in primary subgroup analyses of cerebral microbleeds on MRI and in exploratory subgroup analyses of other features on CT or MRI. The trial is registered with the ISRCTN registry, number ISRCTN71907627.
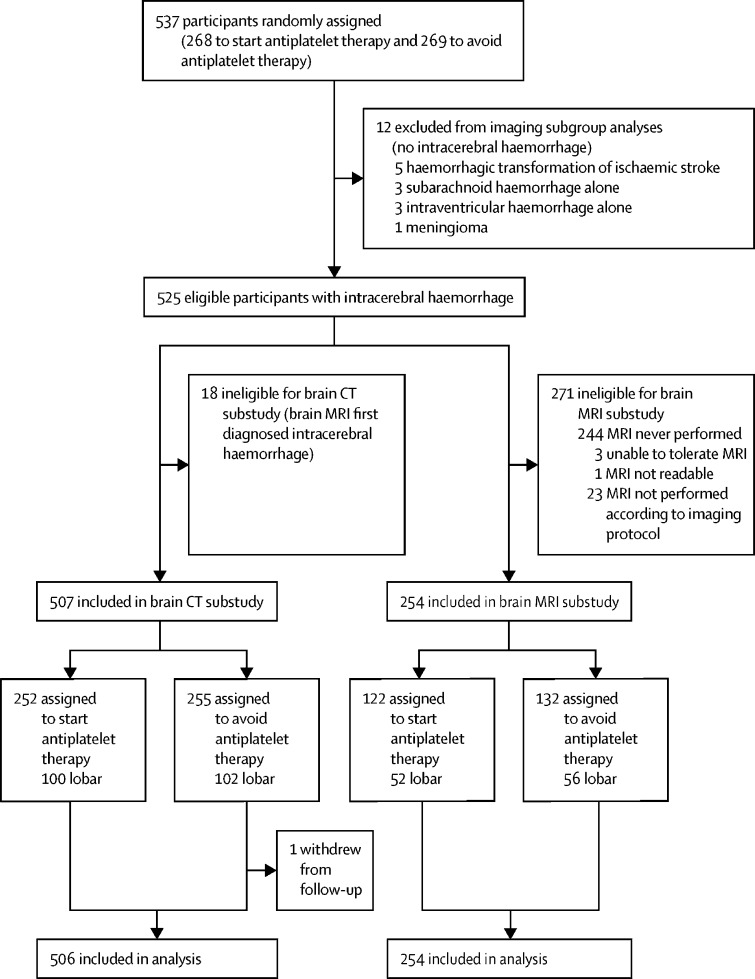
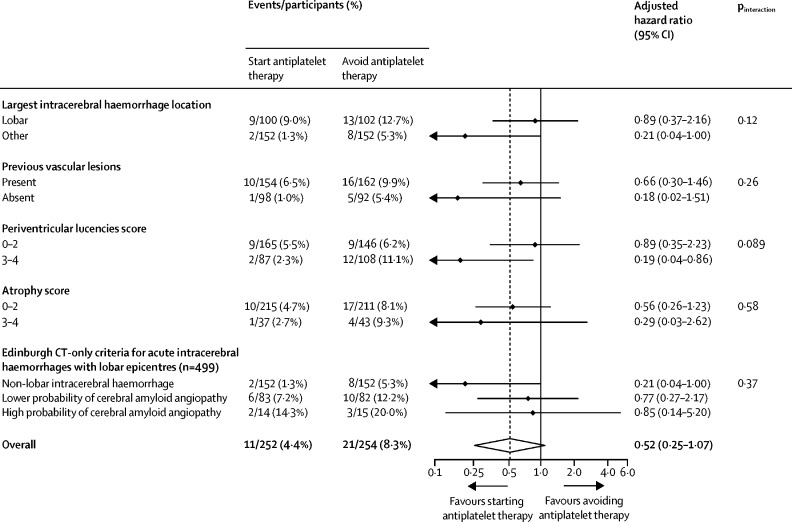
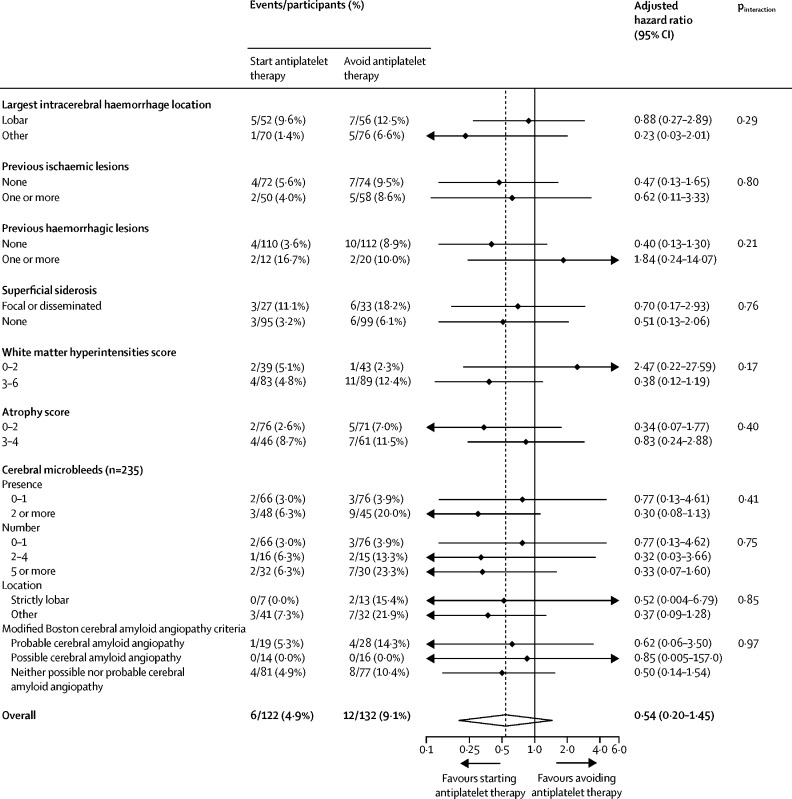
Findings: Between May 22, 2013, and May 31, 2018, 537 participants were enrolled, of whom 525 (98%) had intracerebral haemorrhage: 507 (97%) were diagnosed on CT (252 assigned to start antiplatelet therapy and 255 assigned to avoid antiplatelet therapy, of whom one withdrew and was not analysed) and 254 (48%) underwent the required brain MRI protocol (122 in the start antiplatelet therapy group and 132 in the avoid antiplatelet therapy group). There were no clinically or statistically significant hazards of antiplatelet therapy on recurrent intracerebral haemorrhage in primary subgroup analyses of cerebral microbleed presence (2 or more) versus absence (0 or 1) (adjusted hazard ratio [HR] 0·30 [95% CI 0·08-1·13] vs 0·77 [0·13-4·61]; pinteraction=0·41), cerebral microbleed number 0-1 versus 2-4 versus 5 or more (HR 0·77 [0·13-4·62] vs 0·32 [0·03-3·66] vs 0·33 [0·07-1·60]; pinteraction=0·75), or cerebral microbleed strictly lobar versus other location (HR 0·52 [0·004-6·79] vs 0·37 [0·09-1·28]; pinteraction=0·85). There was no evidence of heterogeneity in the effects of antiplatelet therapy in any exploratory subgroup analyses (all pinteraction>0·05).
Interpretation: Our findings exclude all but a very modest harmful effect of antiplatelet therapy on recurrent intracerebral haemorrhage in the presence of cerebral microbleeds. Further randomised trials are needed to replicate these findings and investigate them with greater precision.
Funding: British Heart Foundation.
Copyright © 2019 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Antiplatelets after intracerebral haemorrhage: treat the patient, not the brain imaging.Lancet Neurol. 2019 Jul;18(7):617-619. doi: 10.1016/S1474-4422(19)30189-9. Epub 2019 May 22. Lancet Neurol. 2019. PMID: 31129066 No abstract available.
References
-
- Qiu J, Ye H, Wang J, Yan J, Wang J, Wang Y. Antiplatelet therapy, cerebral microbleeds, and intracerebral hemorrhage: a meta-analysis. Stroke. 2018;49:1751–1754. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- MR/J006971/1/MRC_/Medical Research Council/United Kingdom
- G0400069/MRC_/Medical Research Council/United Kingdom
- SP/08/010/25939/BHF_/British Heart Foundation/United Kingdom
- PG/14/50/30891/BHF_/British Heart Foundation/United Kingdom
- SP/14/3/31114/BHF_/British Heart Foundation/United Kingdom
- MC_G1002455/MRC_/Medical Research Council/United Kingdom
- CH/09/002/26360/BHF_/British Heart Foundation/United Kingdom
- SCAF/17/01/CSO_/Chief Scientist Office/United Kingdom
- MC_U137686853/MRC_/Medical Research Council/United Kingdom
- MC_UU_12026/5/MRC_/Medical Research Council/United Kingdom
- G0300623/MRC_/Medical Research Council/United Kingdom
- G1002605/MRC_/Medical Research Council/United Kingdom
- SP/12/2/29422/BHF_/British Heart Foundation/United Kingdom
