

Image-based analysis and long-term clinical outcomes of deep brain stimulation for Tourette syndrome: a multisite study
- PMID: 31129620
- PMCID: PMC6744301
- DOI: 10.1136/jnnp-2019-320379
Image-based analysis and long-term clinical outcomes of deep brain stimulation for Tourette syndrome: a multisite study
Abstract
Background: Deep brain stimulation (DBS) can be an effective therapy for tics and comorbidities in select cases of severe, treatment-refractory Tourette syndrome (TS). Clinical responses remain variable across patients, which may be attributed to differences in the location of the neuroanatomical regions being stimulated. We evaluated active contact locations and regions of stimulation across a large cohort of patients with TS in an effort to guide future targeting.
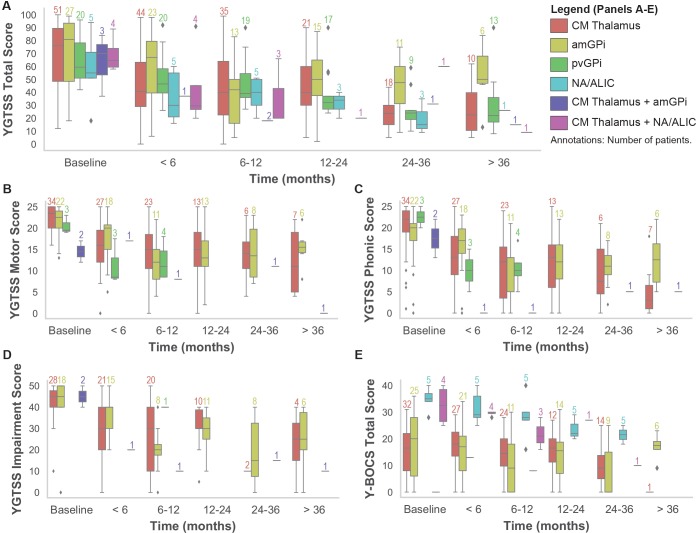
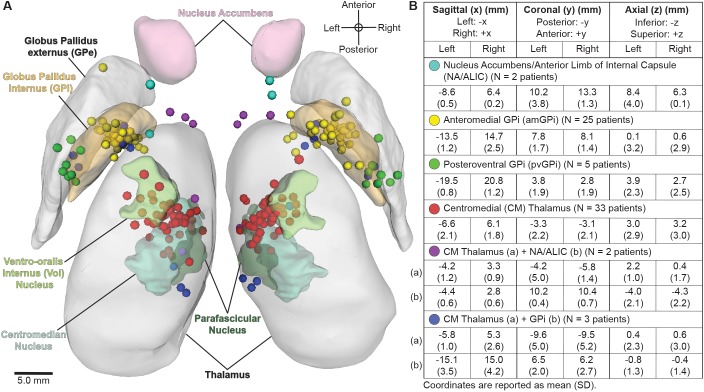
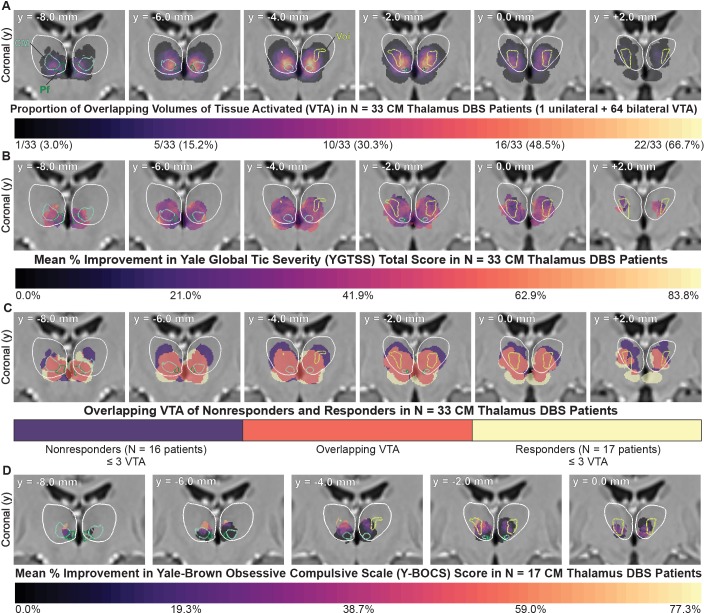
Methods: We collected retrospective clinical data and imaging from 13 international sites on 123 patients. We assessed the effects of DBS over time in 110 patients who were implanted in the centromedial (CM) thalamus (n=51), globus pallidus internus (GPi) (n=47), nucleus accumbens/anterior limb of the internal capsule (n=4) or a combination of targets (n=8). Contact locations (n=70 patients) and volumes of tissue activated (n=63 patients) were coregistered to create probabilistic stimulation atlases.
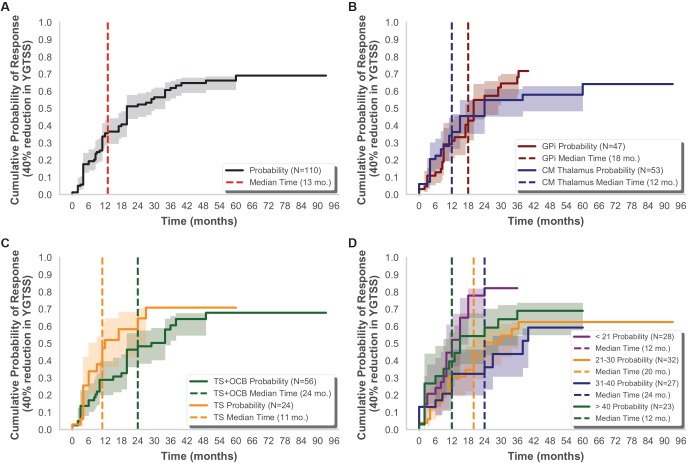
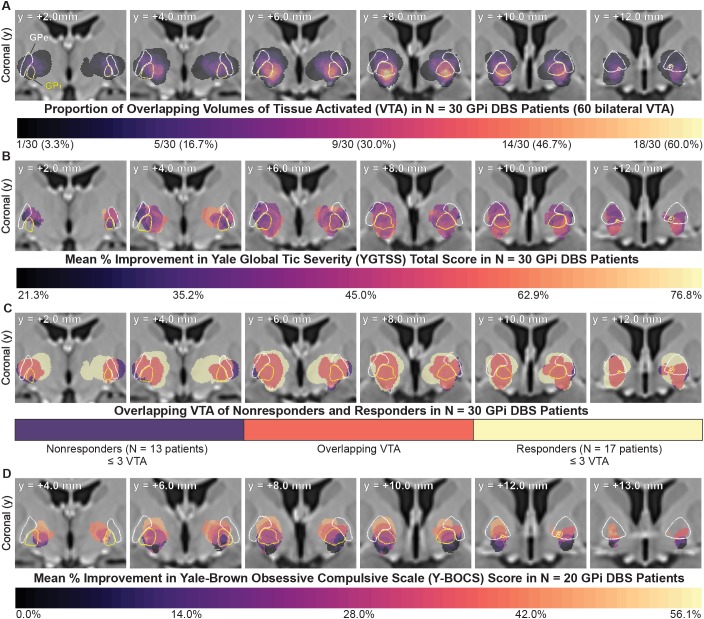
Results: Tics and obsessive-compulsive behaviour (OCB) significantly improved over time (p<0.01), and there were no significant differences across brain targets (p>0.05). The median time was 13 months to reach a 40% improvement in tics, and there were no significant differences across targets (p=0.84), presence of OCB (p=0.09) or age at implantation (p=0.08). Active contacts were generally clustered near the target nuclei, with some variability that may reflect differences in targeting protocols, lead models and contact configurations. There were regions within and surrounding GPi and CM thalamus that improved tics for some patients but were ineffective for others. Regions within, superior or medial to GPi were associated with a greater improvement in OCB than regions inferior to GPi.
Conclusion: The results collectively indicate that DBS may improve tics and OCB, the effects may develop over several months, and stimulation locations relative to structural anatomy alone may not predict response. This study was the first to visualise and evaluate the regions of stimulation across a large cohort of patients with TS to generate new hypotheses about potential targets for improving tics and comorbidities.
Keywords: globus pallidus; neuromodulation; obsessive-compulsive behavior; thalamus; tics.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: JLO has received research grant support from the Michael J Fox Foundation, Boston Scientific, Cala Health, NIH, DARPA, PCORI and Biogen, and she has also received training grant support from Boston Scientific and Medtronic, and has served as a consultant for Acadia Pharmaceuticals and Medtronic. AL serves as a consultant for Boston Scientific and holds intellectual property in the field of DBS. JK has received financial support for investigator-initiated trials from Medtronic and grants from the German Research Foundation (KU2665/1-2) and the Marga and Walter Boll Foundation. CZ has received honoraria and travel expenses from the deep brain stimulation industry (Medtronic, PINS, SceneRay). MSO serves as a consultant for the National Parkinson Foundation, and has received research grants from NIH, NPF, the Michael J Fox Foundation, the Parkinson Alliance, Smallwood Foundation, the Bachmann-Strauss Foundation, the Tourette Syndrome Association, and the UF Foundation. MSO DBS research is supported by R01 NR014852 and R01NS096008. MSO has previously received honoraria, but in the past >60 months has received no support from the industry. MSO has received royalties for publications with Demos, Manson, Amazon, Smashwords, Books4Patients and Cambridge (movement disorders books). MSO is an associate editor for New England Journal of Medicine Journal Watch Neurology. MSO has participated in CME and educational activities on movement disorders (in the last 36 months) sponsored by PeerView, Prime, QuantiaMD, WebMD, Medicus, MedNet, Henry Stewart and by Vanderbilt University. The institution and not MSO receives grants from Medtronic, AbbVie, Allergan and ANS/St Jude, and the PI has no financial interest in these grants. MSO has participated as a site PI and/or co-I for several NIH, foundation and industry sponsored trials over the years but has not received honoraria. CRB has served as a consultant for NeuroPace, Advanced Bionics, Boston Scientific, Intelect Medical, St Jude Medical and Functional Neuromodulation, and he holds intellectual property related to DBS.
Figures
Comment in
-
Deep brain stimulation in Tourette syndrome: the known and the unknown.J Neurol Neurosurg Psychiatry. 2019 Oct;90(10):1076-1077. doi: 10.1136/jnnp-2019-321008. Epub 2019 Jul 12. J Neurol Neurosurg Psychiatry. 2019. PMID: 31300539 Free PMC article. No abstract available.
Similar articles
-
Structural connectivity predicts clinical outcomes of deep brain stimulation for Tourette syndrome.Brain. 2020 Aug 1;143(8):2607-2623. doi: 10.1093/brain/awaa188. Brain. 2020. PMID: 32653920 Free PMC article.
-
Refining the Deep Brain Stimulation Target within the Limbic Globus Pallidus Internus for Tourette Syndrome.Stereotact Funct Neurosurg. 2017;95(4):251-258. doi: 10.1159/000478273. Epub 2017 Aug 5. Stereotact Funct Neurosurg. 2017. PMID: 28787721
-
Deep brain stimulation for Tourette syndrome: a single-center series.J Neurosurg. 2018 Feb;128(2):596-604. doi: 10.3171/2016.10.JNS161573. Epub 2017 Apr 7. J Neurosurg. 2018. PMID: 28387621
-
Deep brain stimulation for Tourette syndrome: target selection.Stereotact Funct Neurosurg. 2012;90(4):213-24. doi: 10.1159/000337776. Epub 2012 Jun 14. Stereotact Funct Neurosurg. 2012. PMID: 22699684 Review.
-
Efficacy of deep brain stimulation for Tourette syndrome and its comorbidities: A meta-analysis.Neurotherapeutics. 2024 Jul;21(4):e00360. doi: 10.1016/j.neurot.2024.e00360. Epub 2024 Apr 30. Neurotherapeutics. 2024. PMID: 38688785 Free PMC article.
Cited by
-
Thalamic Local Field Potentials Are Related to Long-Term DBS Effects in Tourette Syndrome.Front Neurol. 2021 Feb 15;12:578324. doi: 10.3389/fneur.2021.578324. eCollection 2021. Front Neurol. 2021. PMID: 33658970 Free PMC article.
-
Target-Specific Effects of Deep Brain Stimulation for Tourette Syndrome: A Systematic Review and Meta-Analysis.Front Neurol. 2021 Oct 20;12:769275. doi: 10.3389/fneur.2021.769275. eCollection 2021. Front Neurol. 2021. PMID: 34744993 Free PMC article.
-
Tourettic OCD: Current understanding and treatment challenges of a unique endophenotype.Front Psychiatry. 2022 Jul 27;13:929526. doi: 10.3389/fpsyt.2022.929526. eCollection 2022. Front Psychiatry. 2022. PMID: 35966462 Free PMC article. Review.
-
Tics: neurological disorders determined by a deficit in sensorimotor gating processes.Neurol Sci. 2022 Oct;43(10):5839-5850. doi: 10.1007/s10072-022-06235-0. Epub 2022 Jul 4. Neurol Sci. 2022. PMID: 35781754 Free PMC article. Review.
-
European clinical guidelines for Tourette syndrome and other tic disorders-version 2.0. Part IV: deep brain stimulation.Eur Child Adolesc Psychiatry. 2022 Mar;31(3):443-461. doi: 10.1007/s00787-021-01881-9. Epub 2021 Oct 4. Eur Child Adolesc Psychiatry. 2022. PMID: 34605960 Free PMC article. Review.