

Is Long-Segment Fixation a Rule in Fractures Associated With Ankylosing Spondylitis?
- PMID: 31131223
- PMCID: PMC6510176
- DOI: 10.14444/6029
Is Long-Segment Fixation a Rule in Fractures Associated With Ankylosing Spondylitis?
Abstract
Study design: Technical report.
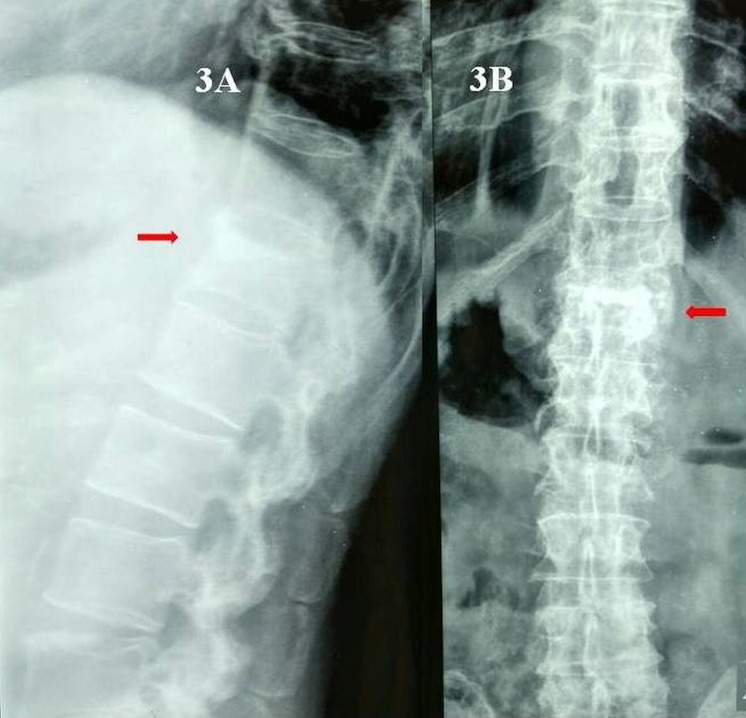
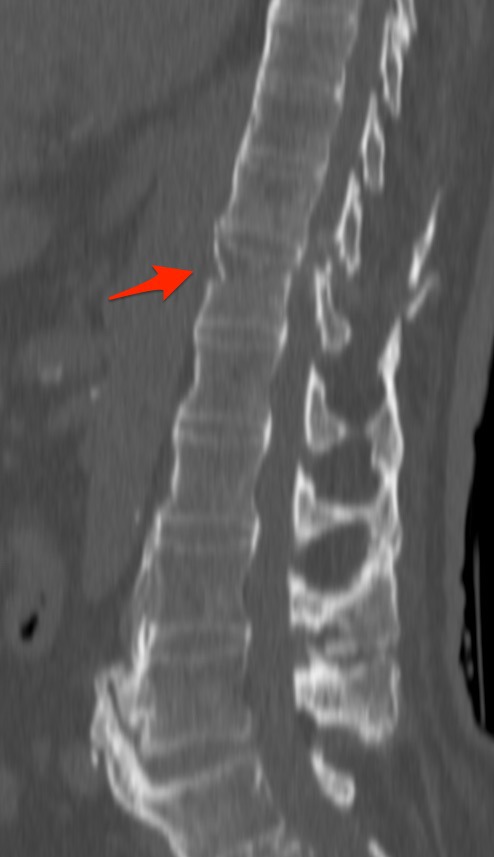
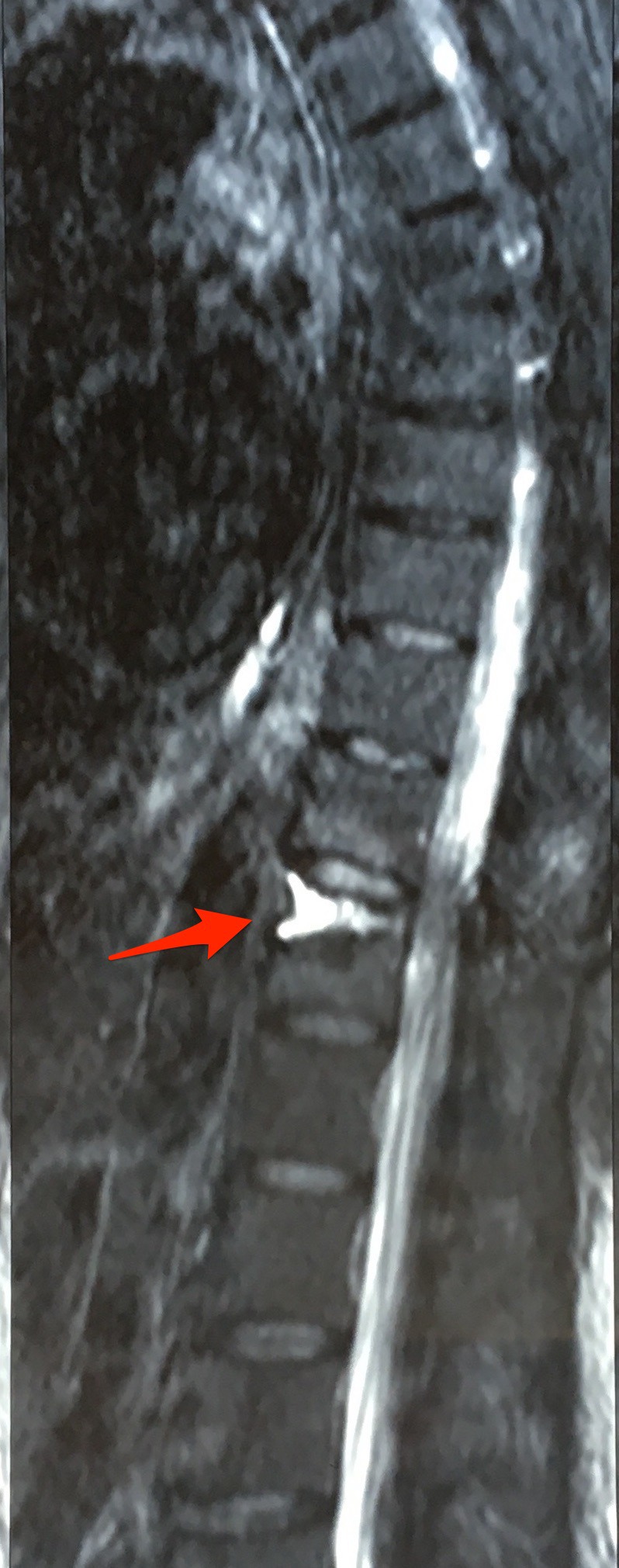
Objective: We describe the outcomes of percutaneous vertebroplasty in 3-columnar thoraco-lumbar fracture secondary to hyper-extension injury in 3 patients with ankylosing spondylitis (AS). Thoraco-lumbar hyperextension injuries in AS are generally unstable as they involve all 3 spinal columns and traditionally require long-segment posterior instrumented stabilization.
Methods: Three cases of AS with severe medical comorbidities underwent percutaneous vertebroplasty for hyper-extension injury involving all 3 columns. Visual analog scale (VAS) and Oswestry Disability Index (ODI) scores were documented preoperatively, postoperatively, and at the last follow-up.
Results: Excellent improvements in VAS and ODI scores were achieved. The patients have no complaints and are independent and mobile at 2 years follow-up.
Conclusion: Vertebroplasty is an excellent option in such medically unfit patients with similar diagnosis and should be performed as early as possible before profound instability or neurological insult sets in, which would necessitate bigger and morbid surgeries.
Keywords: 3 column injuries; ankylosing spondylitis, thoraco-lumbar spine fractures; hyper-extension injury; instability; vertebroplasty.
Conflict of interest statement
Disclosures and COI: There is no conflict of interest among the authors or the institution regarding the manuscript, the scientific work or data collection. The legal regulatory status of the device(s)/drug(s) that is/are the subject of this manuscript is not applicable in our country. No funds were received in support of this work. No benefits in any form have been or will be received from a commercial party related directly or indirectly to the subject of this manuscript. There was no breach of ethical issues by any of the authors mentioned. The manuscript has been read and approved by the authors and each one of the authors treat their work trust worthy within all ethical parameters.
Figures





Similar articles
-
Percutaneous instrumentation with cement augmentation for traumatic hyperextension thoracic and lumbar fractures in ankylosing spondylitis: a single-institution experience.Neurosurg Focus. 2021 Oct;51(4):E8. doi: 10.3171/2021.7.FOCUS21308. Neurosurg Focus. 2021. PMID: 34598149
-
Percutaneous surgery for thoraco-lumbar fractures in ankylosing spondylitis: Study of 31 patients.Orthop Traumatol Surg Res. 2017 Dec;103(8):1235-1239. doi: 10.1016/j.otsr.2017.07.023. Epub 2017 Sep 28. Orthop Traumatol Surg Res. 2017. PMID: 28964918
-
Fracture reduction by postoperative mobilisation for the treatment of hyperextension injuries of the thoracolumbar spine in patients with ankylosing spinal disorders.Arch Orthop Trauma Surg. 2017 Apr;137(4):531-541. doi: 10.1007/s00402-017-2653-7. Epub 2017 Feb 21. Arch Orthop Trauma Surg. 2017. PMID: 28224297 Free PMC article.
-
Management of spinal fractures in patients with ankylosing spondylitis.Clin Neurol Neurosurg. 2015 Dec;139:177-82. doi: 10.1016/j.clineuro.2015.10.014. Epub 2015 Oct 23. Clin Neurol Neurosurg. 2015. PMID: 26513429 Review.
-
Comparison of Percutaneous Vertebroplasty and Balloon Kyphoplasty for the Treatment of Single Level Vertebral Compression Fractures: A Meta-analysis of the Literature.Pain Physician. 2015 May-Jun;18(3):209-22. Pain Physician. 2015. PMID: 26000665 Review.
Cited by
-
Case series: O-arm navigation assisted by the Wiltse approach improves the accuracy of pedicle screw placement in ankylosing spondylitis combined with thoracolumbar fractures.Medicine (Baltimore). 2023 Dec 29;102(52):e36807. doi: 10.1097/MD.0000000000036807. Medicine (Baltimore). 2023. PMID: 38206734 Free PMC article.
-
Standalone Percutaneous Vertebroplasty for Hyperextension Injuries of the Ankylosed Thoracolumbar Spinal Kyphosis.Asian Spine J. 2023 Dec;17(6):1132-1138. doi: 10.31616/asj.2023.0113. Epub 2023 Dec 18. Asian Spine J. 2023. PMID: 38105639 Free PMC article.
-
Kyphoplasty for thoracic and lumbar fractures with an intravertebral vacuum phenomenon in ankylosing spondylitis patients.Front Surg. 2022 Jul 29;9:962723. doi: 10.3389/fsurg.2022.962723. eCollection 2022. Front Surg. 2022. PMID: 35965876 Free PMC article.
-
Percutaneous kyphoplasty for the treatment of diffuse idiopathic skeletal hyperostosis with vertebral fractures: A case report and treatment review.Front Surg. 2022 Jul 15;9:922139. doi: 10.3389/fsurg.2022.922139. eCollection 2022. Front Surg. 2022. PMID: 35910472 Free PMC article.
-
Surgical Treatment of Andersson Lesion of the Lumbar Spine with Minimal Invasion: A Case Report.Orthop Surg. 2022 Nov;14(11):3129-3133. doi: 10.1111/os.13426. Epub 2022 Sep 29. Orthop Surg. 2022. PMID: 36172923 Free PMC article.
References
-
- Davey-Ranasinghe N, Deodhar A. Osteoporosis and vertebral fractures in ankylosing spondylitis. Curr Opin Rheumatol. 2013;25(4):509–516. - PubMed
-
- Calin A, Fries JF. Striking prevalence of ankylosing spondylitis in “healthy” HLAB27 positive males and females. N Engl J Med. 1975;293(17):835–839. - PubMed
-
- Westerveld LA, van Bemmel JC, Dhert WJA, Oner FC, Verlaan JJ. Clinical outcome after traumatic spinal fractures in patients with ankylosing spinal disorders compared with control patients. Spine J. 2014;14(5):729–740. - PubMed
-
- Braun J, Sieper J. Ankylosing spondylitis. Lancet. 2007;369(9570):1379–1390. - PubMed
-
- Bouxsein ML, Melton LJ, Riggs BL, et al. Age-and sex-specific differences in the factor of risk for vertebral fracture: a population-based study using QCT. J Bone Min Res. 2006;21(9):1475–1482. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials