

Long-Dose Intensive Therapy Is Necessary for Strong, Clinically Significant, Upper Limb Functional Gains and Retained Gains in Severe/Moderate Chronic Stroke
- PMID: 31131743
- PMCID: PMC6625035
- DOI: 10.1177/1545968319846120
Long-Dose Intensive Therapy Is Necessary for Strong, Clinically Significant, Upper Limb Functional Gains and Retained Gains in Severe/Moderate Chronic Stroke
Abstract
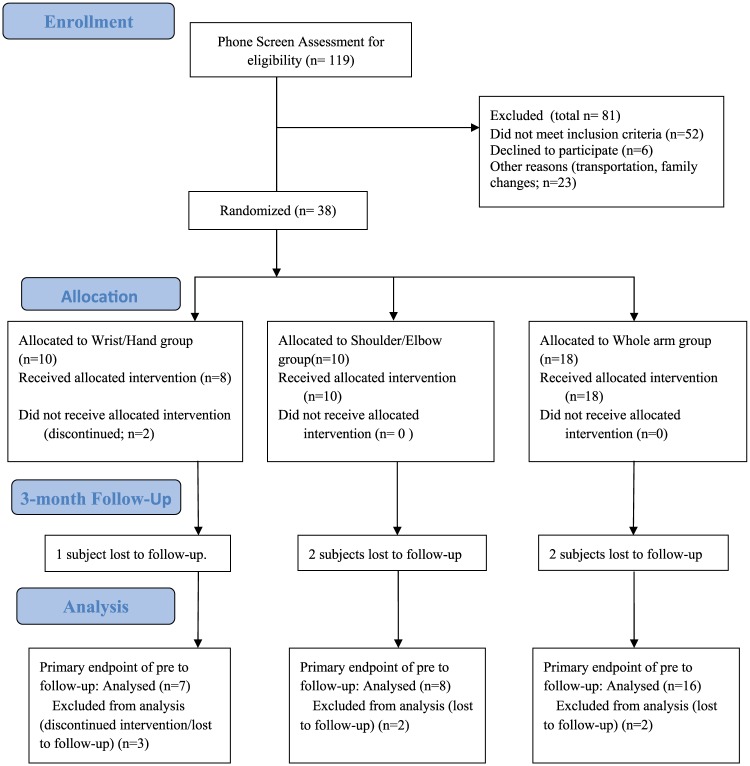
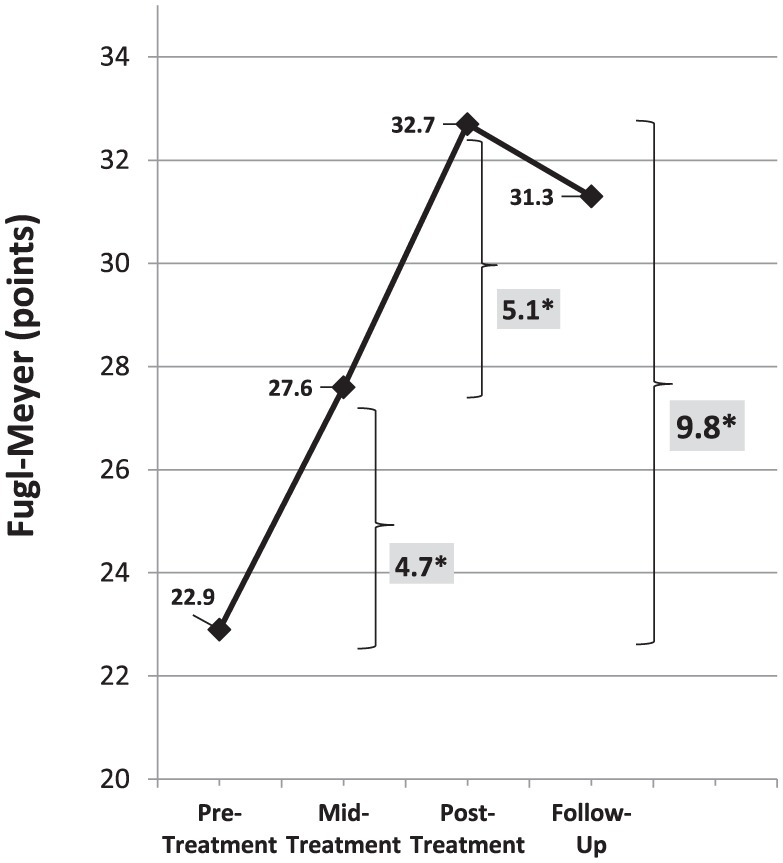
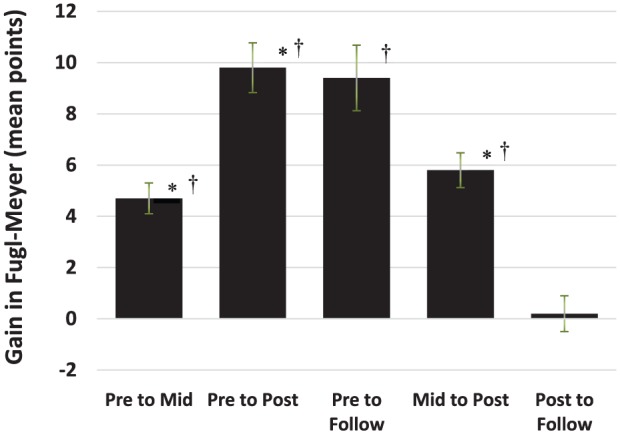
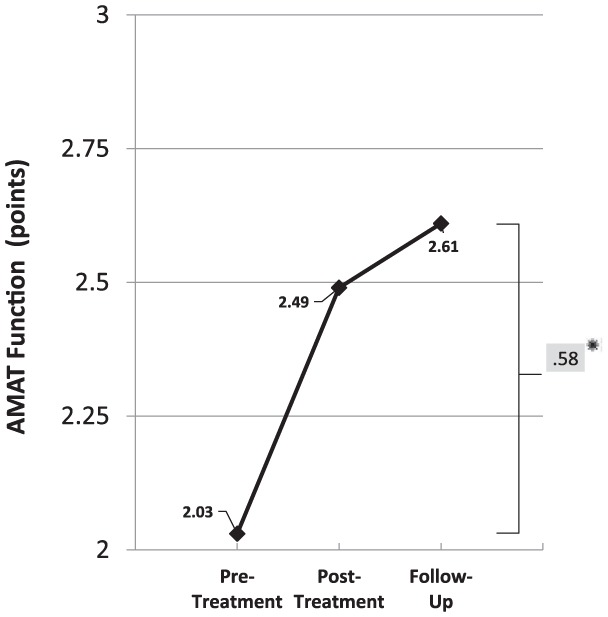
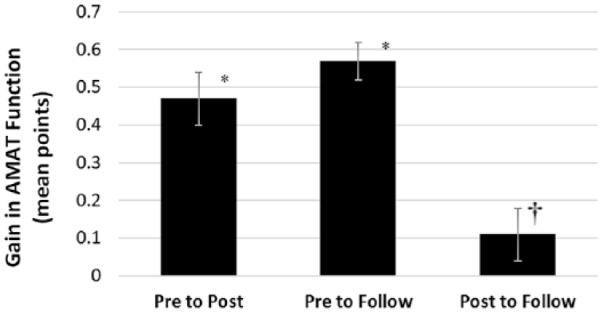
Background. Effective treatment methods are needed for moderate/severely impairment chronic stroke. Objective. The questions were the following: (1) Is there need for long-dose therapy or is there a mid-treatment plateau? (2) Are the observed gains from the prior-studied protocol retained after treatment? Methods. Single-blind, stratified/randomized design, with 3 applied technology treatment groups, combined with motor learning, for long-duration treatment (300 hours of treatment). Measures were Arm Motor Ability Test time and coordination-function (AMAT-T, AMAT-F, respectively), acquired pre-/posttreatment and 3-month follow-up (3moF/U); Fugl-Meyer (FM), acquired similarly with addition of mid-treatment. Findings. There was no group difference in treatment response (P ≥ .16), therefore data were combined for remaining analyses (n = 31; except for FM pre/mid/post, n = 36). Pre-to-Mid-treatment and Mid-to-Posttreatment gains of FM were statistically and clinically significant (P < .0001; 4.7 points and P < .001; 5.1 points, respectively), indicating no plateau at 150 hours and benefit of second half of treatment. From baseline to 3moF/U: (1) FM gains were twice the clinically significant benchmark, (2) AMAT-F gains were greater than clinically significant benchmark, and (3) there was statistically significant improvement in FM (P < .0001); AMAT-F (P < .0001); AMAT-T (P < .0001). These gains indicate retained clinically and statistically significant gains at 3moFU. From posttreatment to 3moF/U, gains on FM were maintained. There were statistically significant gains in AMAT-F (P = .0379) and AMAT-T P = .003.
Keywords: coordination; function; rehabilitation; stroke; upper limb.
Conflict of interest statement
Figures


References
-
- Winstein CJ, Stein J, Arena R, et al. Guidelines for adult stroke rehabilitation and recovery: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2016;47:e98-e169. - PubMed
-
- Hayward K, Barker R, Brauer S. Interventions to promote upper limb recovery in stroke survivors with severe paresis: systematic review. Disabil Rehabil. 2010;32:1973-1986. - PubMed
-
- Lin KC, Chen YA, Chen CL, Wu CY, Chang YF. Effects of bilateral arm training on motor control and functional performance in chronic stroke: randomized controlled study. Neurorehabil Neural Repair. 2010;24:42-51. - PubMed
-
- Lin KC, Wu CY, Liu JS, Chen YT, Hsu CJ. Constraint-induced therapy versus dose-matched control intervention to improve motor ability, basic/extended daily functions, and quality of life in stroke. Neurorehabil Neural Repair. 2009;23:160-165. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
