

Review
doi: 10.1161/HYPERTENSIONAHA.119.12992.
Epub 2019 May 28.
Pulmonary Hypertension and ATP-Sensitive Potassium Channels
Affiliations
- PMID: 31132951
- PMCID: PMC6561811
- DOI: 10.1161/HYPERTENSIONAHA.119.12992
Item in Clipboard
Review
Pulmonary Hypertension and ATP-Sensitive Potassium Channels
Hypertension.
2019 Jul.
No abstract available
Conflict of interest statement
The authors have declared that no conflict of interest exists.
Figures
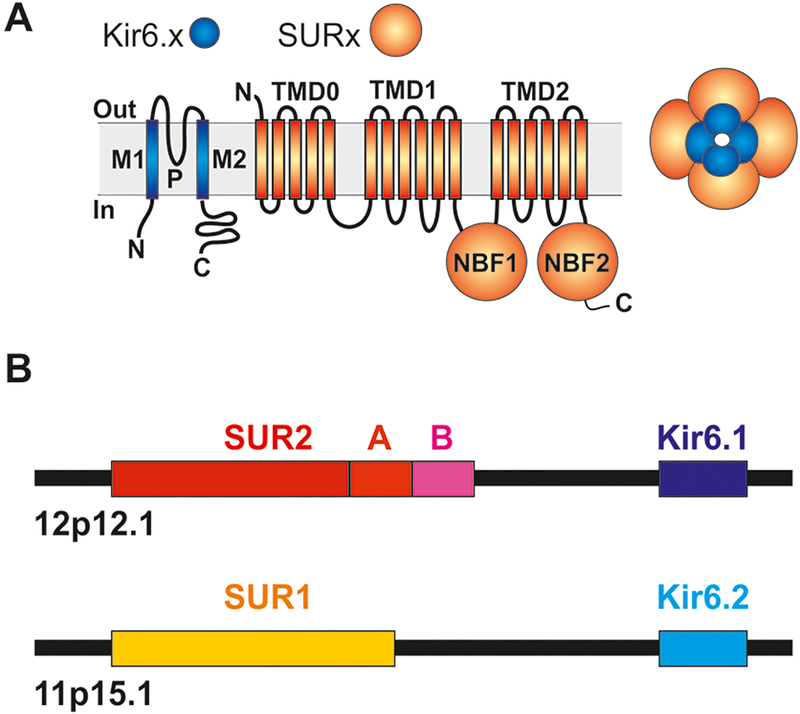
(A) KATP channels are generated as octamers of 4 pore-forming Kir6.x (Kir6.1 or Kir6.2) and 4 regulatory SURx (SUR1 or SUR2) subunits. (B) Two pairs of genes located on human chromosome 12 (ABCC9, KCNJ8) and chromosome 11 (ABCC8, KCNJ11) encode SUR2 (C-terminally spliced to SUR2A or SUR2B) and Kir6.1, or SUR1 and Kir6.2 subunits, respectively.
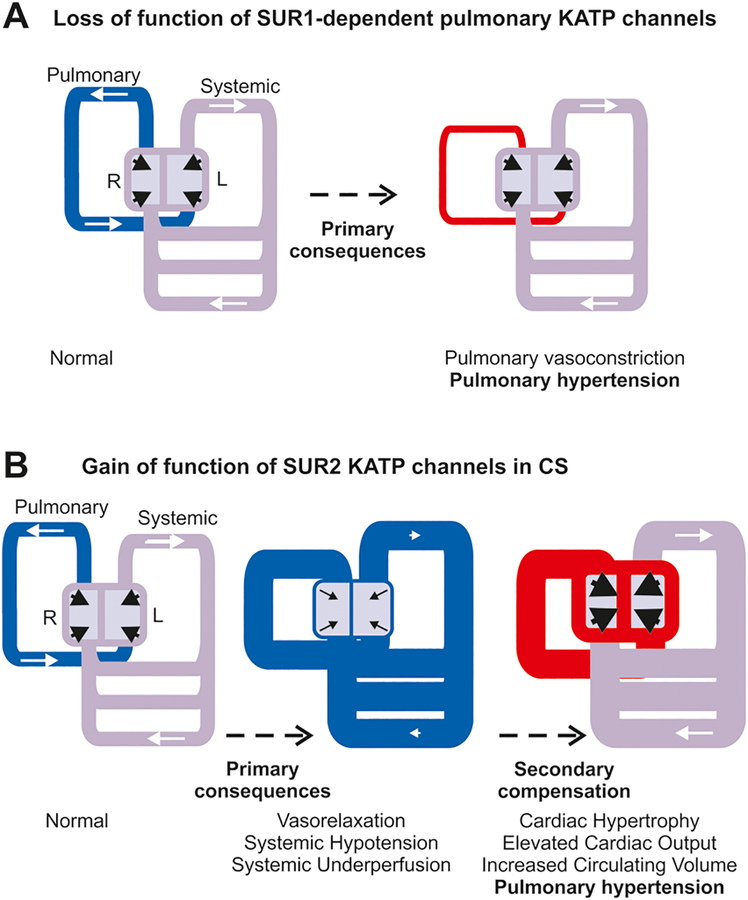
(A) Schematic of cardiovascular system indicates normal pressures (grey) in systemic circulation and low pressures (blue) in pulmonary circulation resulting from normal pumping from the left (L) and right (R) heart, respectively. Loss-of-function of SUR1-dependent KATP (or other K) channels in pulmonary circulation may directly result in inappropriate pulmonary vasoconstriction and hypertension (red). (B) Gain-of-function of SUR2-dependent KATP (or other K) channels results primarily in inappropriate vasorelaxation and systemic hypotension (blue). Secondary compensatory mechanisms drive enlarged, hypercontractile hearts, raising pressures in the systemic circulation (to normal, grey) and in the pulmonary circulation (to hypertension, red).
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
