

Antihypertensive Medication Nonpersistence and Low Adherence for Adults <65 Years Initiating Treatment in 2007-2014
- PMID: 31132956
- PMCID: PMC6914333
- DOI: 10.1161/HYPERTENSIONAHA.118.12495
Antihypertensive Medication Nonpersistence and Low Adherence for Adults <65 Years Initiating Treatment in 2007-2014
Abstract
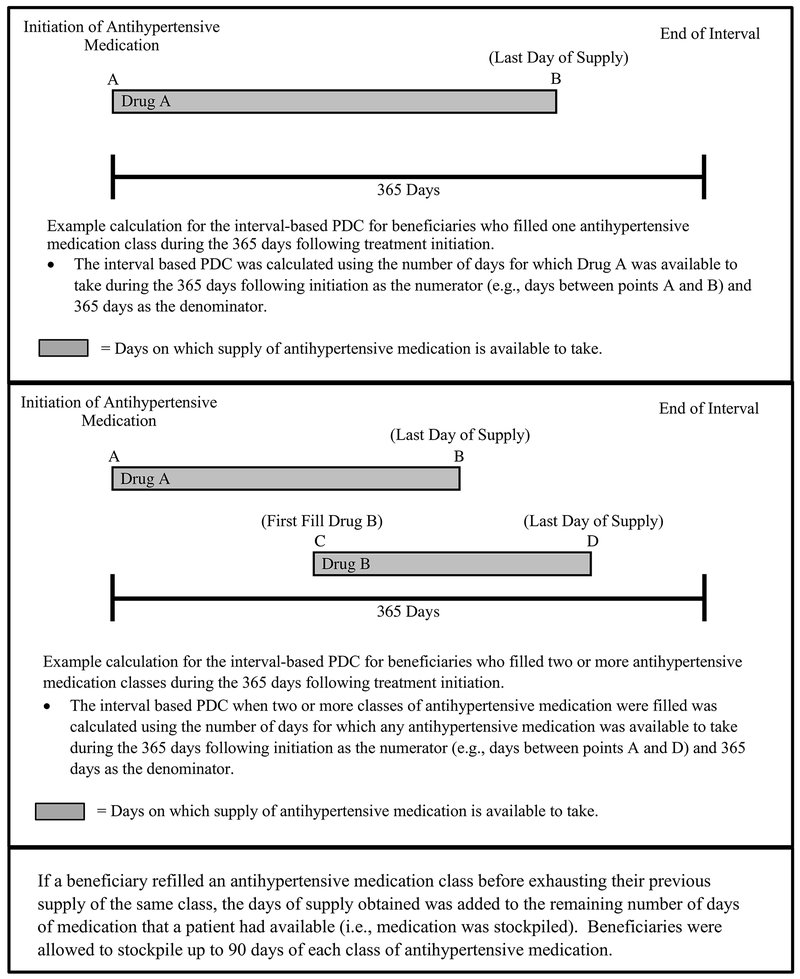
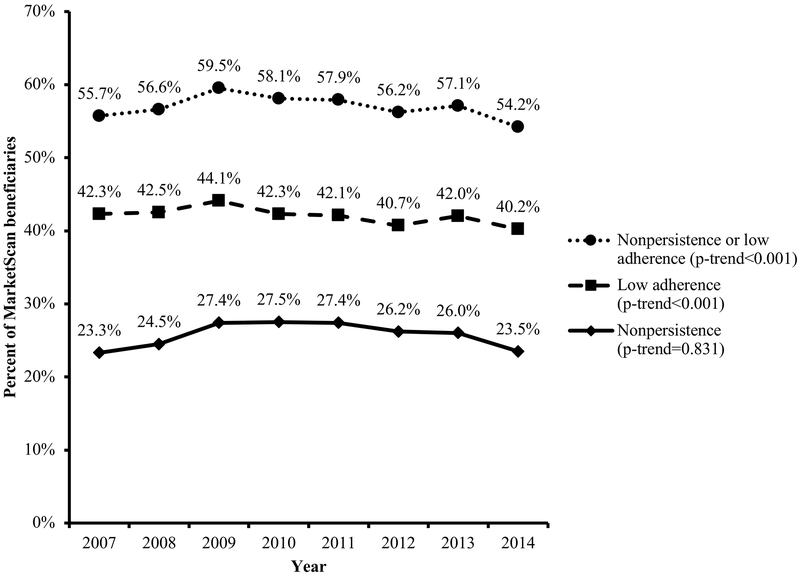
Previous evidence suggests modest improvements in antihypertensive medication adherence occurred from 2007 to 2012 among US adults ≥65 years of age. Whether adherence improved over time among adults <65 years of age is unknown. We assessed trends in antihypertensive medication nonpersistence and low adherence among 379 658 commercially insured adults <65 years of age initiating treatment in 2007-2014 using MarketScan claims. Nonpersistence was defined as having no days of medication available to take during the final 90 days of the 365 days following initiation. Among beneficiaries who were persistent to treatment, low adherence was defined by having antihypertensive medication available to take for <80% of the days in the 365 days following initiation (ie, proportion of days covered <80%). In 2007 and 2014, 23.3% and 23.5% of patients were nonpersistent to treatment, respectively, and 42.3% and 40.2% had low adherence, respectively. The relative risks for nonpersistence and low adherence were lower among beneficiaries initiating treatment with an angiotensin-converting enzyme inhibitor (0.95; 95% CI, 0.94-0.97 and 0.97; 95% CI, 0.96-0.98, respectively), angiotensin receptor blocker (0.86; 95% CI, 0.85-0.88 and 0.99; 95% CI, 0.97-1.00, respectively), or multiclass regimen (0.82; 95% CI, 0.80-0.84 and 0.88; 95% CI, 0.86-0.89, respectively), prescribed 90-day versus 30-day prescriptions (0.67; 95% CI, 0.66-0.68 and 0.70; 95% CI, 0.69-0.71, respectively), or who received medications by mail versus at the pharmacy (0.93; 95% CI, 0.90-0.95 and 0.90; 95% CI, 0.88-0.92, respectively). In conclusion, several modifiable factors were associated with lower rates of both antihypertensive medication nonpersistence and low adherence among adults <65 years of age initiating treatment in 2007-2014.
Keywords: epidemiology; hypertension; medication adherence; risk factors.
Figures
Comment in
-
Improving Blood Pressure Control in the Hypertensive Population.Hypertension. 2019 Jul;74(1):29-31. doi: 10.1161/HYPERTENSIONAHA.119.12598. Epub 2019 May 28. Hypertension. 2019. PMID: 31132950 No abstract available.
References
-
- Staessen JA, Wang JG, Thijs L. Cardiovascular protection and blood pressure reduction: a meta-analysis. Lancet. Oct 20 2001;358(9290):1305–1315. - PubMed
-
- Ho PM, Bryson CL, Rumsfeld JS. Medication adherence: its importance in cardiovascular outcomes. Circulation. Jun 16 2009;119(23):3028–3035. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- T32 HS013852/HS/AHRQ HHS/United States
- P20 GM109036/GM/NIGMS NIH HHS/United States
- R01 HL133790/HL/NHLBI NIH HHS/United States
- K01 HL133468/HL/NHLBI NIH HHS/United States
- UL1 TR003096/TR/NCATS NIH HHS/United States
- R21 LM012448/LM/NLM NIH HHS/United States
- KL2 TR002015/TR/NCATS NIH HHS/United States
- R01 HS024262/HS/AHRQ HHS/United States
- K12 HD043451/HD/NICHD NIH HHS/United States
- K12 AR084224/AR/NIAMS NIH HHS/United States
- U54 GM104940/GM/NIGMS NIH HHS/United States
- T32 HL007457/HL/NHLBI NIH HHS/United States
- R01 DK108628/DK/NIDDK NIH HHS/United States
- R01 HL123368/HL/NHLBI NIH HHS/United States
- R01 HL130500/HL/NHLBI NIH HHS/United States
- UL1 TR002014/TR/NCATS NIH HHS/United States
- UL1 TR001417/TR/NCATS NIH HHS/United States
- K24 HL125704/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
