

Equitable realization of the right to health in Haiti: how household data inform health seeking behavior and financial risk protection
- PMID: 31133035
- PMCID: PMC6537186
- DOI: 10.1186/s12939-019-0973-7
Equitable realization of the right to health in Haiti: how household data inform health seeking behavior and financial risk protection
Abstract
Background: Though the right to health is included in Haiti's constitution, little progress has been made to expand universal health coverage nationwide, a strategy to ensure access to health services for all, while preventing financial hardship among the poor. Realizing universal health coverage will require a better understanding of inequities in health care utilization and out-of-pocket payments for health. This study measures inequality in health services utilization and the determinants of health seeking behavior in Haiti. It also examines the determinants of catastrophic health expenditures, defined by the Sustainable Development Goal Framework (Indicator 3.8.2) as expenditures that exceed 10% of overall household expenditures.
Methodology: Three types of analysis were conducted using the 2012 and 2013 Household Surveys (Enquête sur les Conditions de Vie des Ménages Après Séisme (ECVMAS I (2012) and ECVMAS II (2013)) to measure: 1) outpatient services as a measure of inequalities using the 2013 Concentration Index; 2) drivers of health seeking behavior using a logistic regression model for 2013; and 3) determinants of catastrophic health expenditures using Seemingly Unrelated Regressions for both 2012 and 2013.
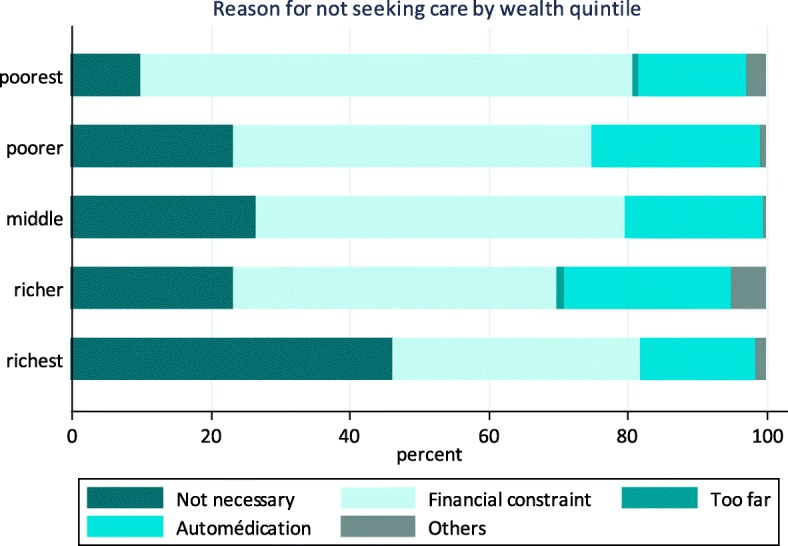
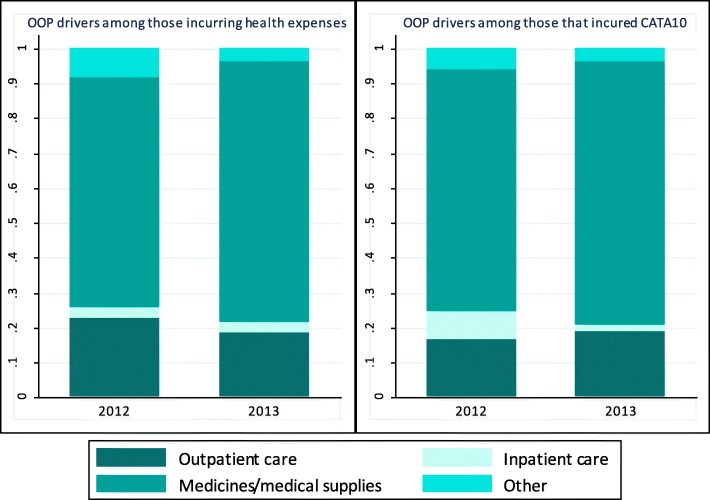
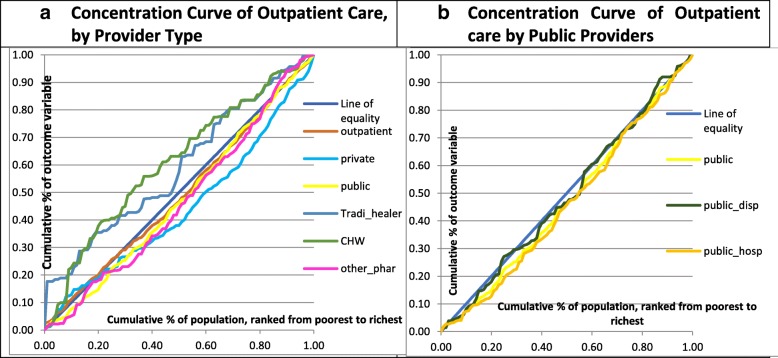
Results: The rate of catastrophic health expenditures increased nationwide from 9.43% in 2012 to 11.54% in 2013. This increase was most notable among the poorest wealth quintile (from 11.62% in 2012 to 18.20% in 2013), yet declined among the richest wealth quintile (from 9.49% to 4.46% during the same period). The increase in the rate of catastrophic health expenditures among the poorest coincides with a sharp decrease in external donor funding for the health sector. Regression analysis indicated that the rich wealth quintiles were less likely than poor wealth quintiles to incur catastrophic health expenditures. Interestingly, households were less likely to incur catastrophic health expenditures when they accessed care from Community Health Workers than when they received care from other types of providers, including public and private health care facilities. This study also shows that Community Health Worker-provided services have a negative concentration index (- 0.22) and are therefore most utilized by poor quintiles. In contrast, both public and private outpatient services had positive concentration indexes (0.05 and 0.12 respectively) and are most utilized by the rich wealth quintiles. Seeking care from traditional healers was found to be pro-poor in Haiti (concentration index of - 0.18) yet was also associated with higher catastrophic health expenditures albeit the coefficient was not significant.
Conclusion: The expansion of universal health coverage in Haiti is evolving in a 'pro-rich' manner. Realizing Haiti's right to health will require a course-correction supported by national policies that protect the poor wealth quintiles from catastrophic health expenditures. Such policies may include Community Health Worker service delivery expansion in underserved areas. Evidence-based interventions may also be required to lower outpatient user fees, subsidize drug costs and promote efficiencies in pro-poor disaster relief programming.
Keywords: Catastrophic health expenditures (CHE); Disaster relief; Health seeking behavior; Inequalities.
Conflict of interest statement
The author declares that he has no competing interests.
Figures
References
-
- World Health Organization | Health systems financing: the path to universal coverage. WHO; 2010. Available from: http://www.who.int/whr/2010/en/. [cited 2019 Feb 6]. - PMC - PubMed
-
- World Health Organization. Anchoring universal health coverage in the right to health: WHO; 2015. Available from: http://www.who.int/gender-equity-rights/knowledge/anchoring-uhc/en/. [cited 2019 Feb 6]
-
- Human rights and health. 2017. Available from: https://www.who.int/news-room/fact-sheets/detail/human-rights-and-health. [cited 2019 Feb 6]
-
- World Health Organization | Tracking universal health coverage: 2017 global monitoring report. WHO; 2017. Available from: http://www.who.int/healthinfo/universal_health_coverage/report/2017/en/. [cited 2019 Feb 6]
MeSH terms
LinkOut - more resources
Full Text Sources
