

Oncological safety of intrafascial nerve-sparing radical prostatectomy compared with conventional process: a pooled review and meta-regression analysis based on available studies
- PMID: 31133039
- PMCID: PMC6537360
- DOI: 10.1186/s12894-019-0476-2
Oncological safety of intrafascial nerve-sparing radical prostatectomy compared with conventional process: a pooled review and meta-regression analysis based on available studies
Abstract
Background: Intrafascial prostatectomy was a modified technique from the conventional nerve-sparing surgery in order to improve patients' post-surgical continence and erectile function; however, ongoing controversy exists regarding the oncological safety of this technique. In this study we aimed to provide a critical and pooled analysis based on published literatures regarding the oncological outcomes after intrafascial nerve-sparing prostatectomy.
Methods: Database searches were performed for published articles till June 2018 on PubMed. Three reviewers screened fulfilled papers and extracted data independently. Main outcome was the positive surgical margins (PSMs) rates stratified by pathological stages. We performed both one-arm and comparative meta-analysis to evaluate the oncological safety of intrafascial technique. Moreover, we built meta-regression models to assess the confounding factors.
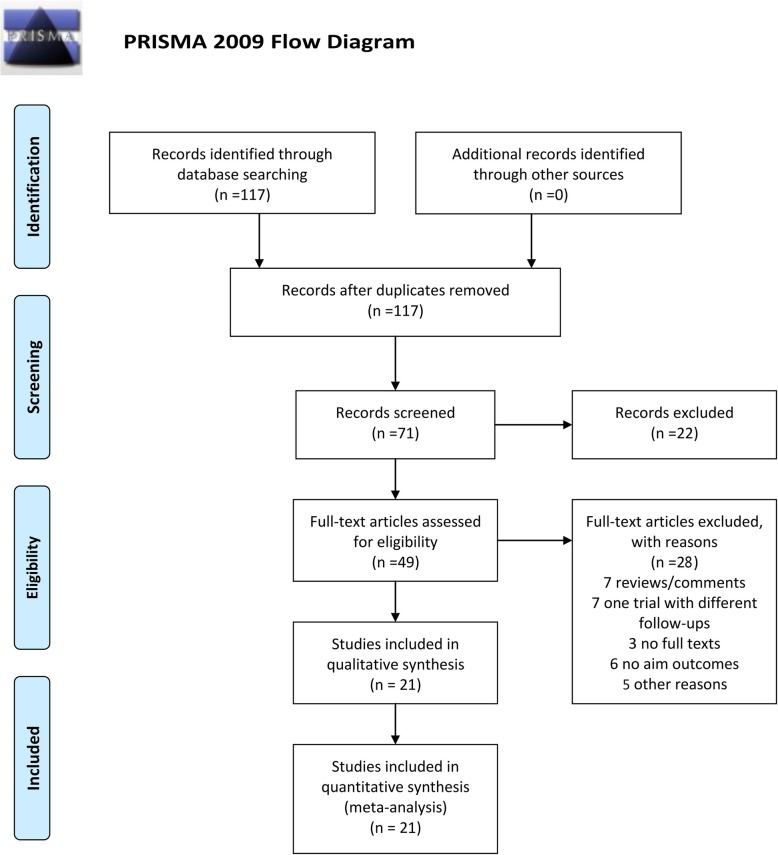
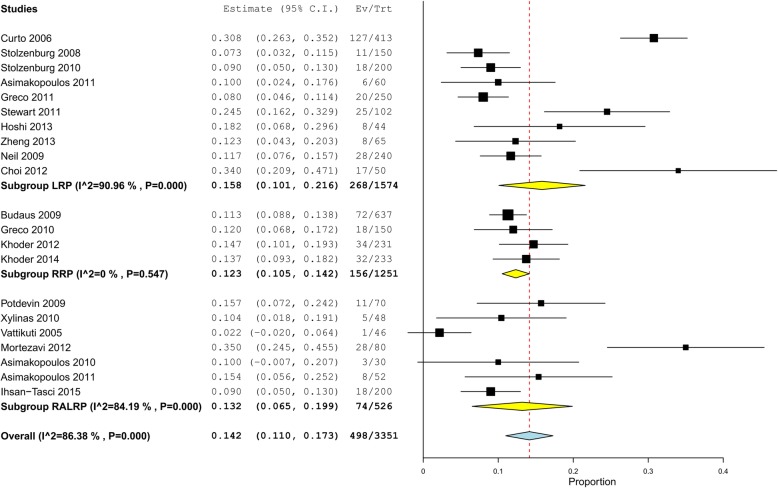
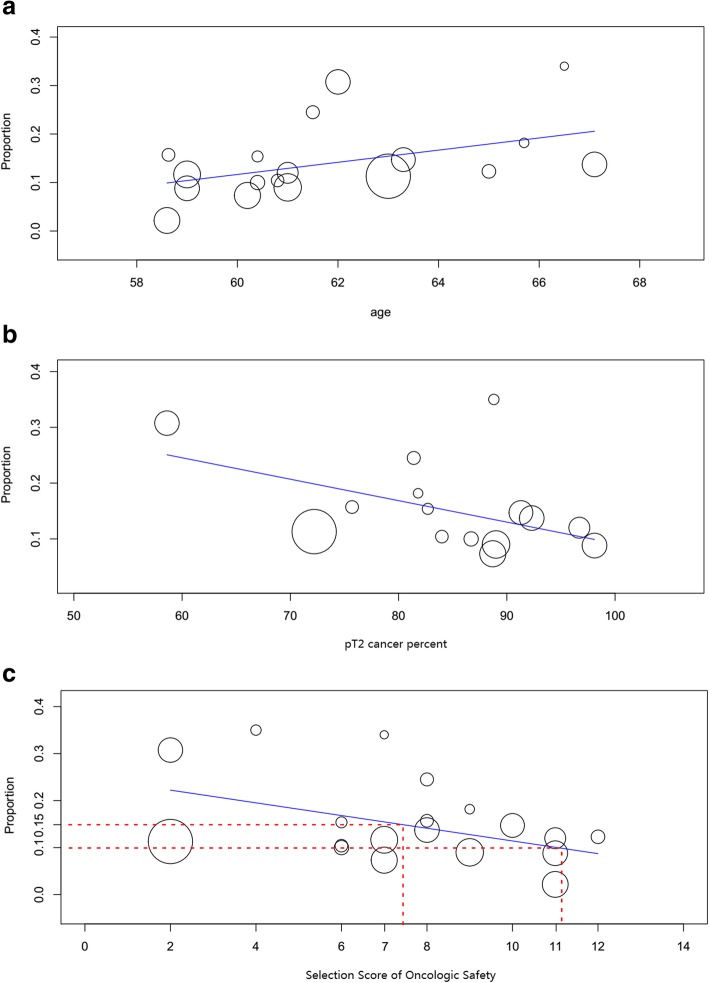
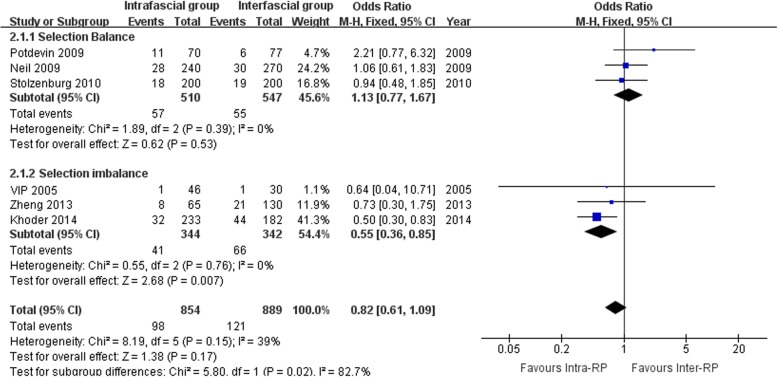
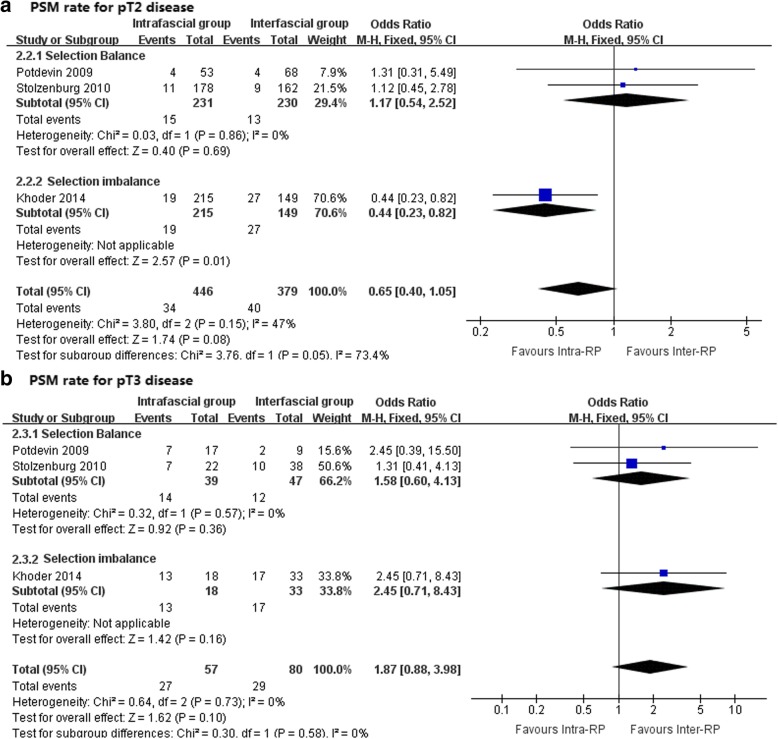
Results: We retrieved a total of 117 records after electronic search, of which 21 studies were finally included in this review. There were 15 controlled studies and 6 surgical series. Our one-arm meta-analysis demonstrated that the total PSM rates after intrafascial techniques ranging from 2.2 to 35%, with a pooled rate of 14.5% on average (480 of 3151 patients, 95% confidence interval[CI]: 11.2-17.5%). Meta-regression model showed that patients' age, pT2 cancer percentage and Selection Score of Oncological Safety (SSOS) were significantly associated with total PSM rate; moreover, each 1 point of SSOS could decrease the total PSM rate by 1.3% on average. Comparative meta-analysis demonstrated that there was no significant difference between intra- and inter-fascial group regarding PSM rates.
Conclusions: With stringent case selection and when performed by experienced surgeons, intrafascial prostatectomy could offer an acceptable or, at least, equivalent PSM rate compared with the conventional interfascial approach. Preoperative SSOS more than 7 points could be considered as an indication of intrafascial radical prostatectomy.
Keywords: Intrafascial nerve-sparing; Oncological safety; Positive surgical margins; Radical prostatectomy; Systematic review.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Intrafascial nerve-sparing radical prostatectomy improves patients' postoperative continence recovery and erectile function: A pooled analysis based on available literatures.Medicine (Baltimore). 2018 Jul;97(29):e11297. doi: 10.1097/MD.0000000000011297. Medicine (Baltimore). 2018. PMID: 30024505 Free PMC article. Review.
-
A matched-pair comparison between bilateral intrafascial and interfascial nerve-sparing techniques in extraperitoneal laparoscopic radical prostatectomy.Asian J Androl. 2013 Jul;15(4):513-7. doi: 10.1038/aja.2012.157. Epub 2013 May 27. Asian J Androl. 2013. PMID: 23708458 Free PMC article. Clinical Trial.
-
Functional and oncologic outcomes comparing interfascial and intrafascial nerve sparing in robot-assisted laparoscopic radical prostatectomies.J Endourol. 2009 Sep;23(9):1479-84. doi: 10.1089/end.2009.0369. J Endourol. 2009. PMID: 19694530
-
Do we need the nerve sparing radical prostatectomy techniques (intrafascial vs. interfascial) in men with erectile dysfunction? Results of a single-centre study.World J Urol. 2015 Mar;33(3):301-7. doi: 10.1007/s00345-014-1302-9. Epub 2014 Apr 22. World J Urol. 2015. PMID: 24752607
-
Intrafascial versus interfascial nerve sparing in radical prostatectomy for localized prostate cancer: a systematic review and meta-analysis.Sci Rep. 2017 Sep 13;7(1):11454. doi: 10.1038/s41598-017-11878-7. Sci Rep. 2017. PMID: 28904361 Free PMC article.
Cited by
-
Penile fracture after nerve-sparing radical prostatectomy: Case report and review of literature.IJU Case Rep. 2025 Feb 10;8(3):198-201. doi: 10.1002/iju5.70004. eCollection 2025 May. IJU Case Rep. 2025. PMID: 40336735 Free PMC article.
-
Different Nerve-Sparing Techniques during Radical Prostatectomy and Their Impact on Functional Outcomes.Cancers (Basel). 2022 Mar 22;14(7):1601. doi: 10.3390/cancers14071601. Cancers (Basel). 2022. PMID: 35406373 Free PMC article. Review.
-
Modified completely intrafascial radical cysprostatectomy for bladder cancer: a single-center, blinded, controlled study.BMC Cancer. 2021 Aug 3;21(1):887. doi: 10.1186/s12885-021-08568-z. BMC Cancer. 2021. PMID: 34340675 Free PMC article. Clinical Trial.
-
Comparative Analysis of Cold Versus Thermal Dissection in Nerve-Sparing Robot-Assisted Radical Prostatectomy.Cancers (Basel). 2025 May 30;17(11):1831. doi: 10.3390/cancers17111831. Cancers (Basel). 2025. PMID: 40507309 Free PMC article.
-
Robotic radical prostatectomy: analysis of midterm pathologic and oncologic outcomes: A historical series from a high-volume center.Surg Endosc. 2021 Dec;35(12):6731-6745. doi: 10.1007/s00464-020-08177-0. Epub 2020 Dec 7. Surg Endosc. 2021. PMID: 33289056 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
