

Mother-to-Child HTLV-1 Transmission: Unmet Research Needs
- PMID: 31134031
- PMCID: PMC6517543
- DOI: 10.3389/fmicb.2019.00999
Mother-to-Child HTLV-1 Transmission: Unmet Research Needs
Abstract
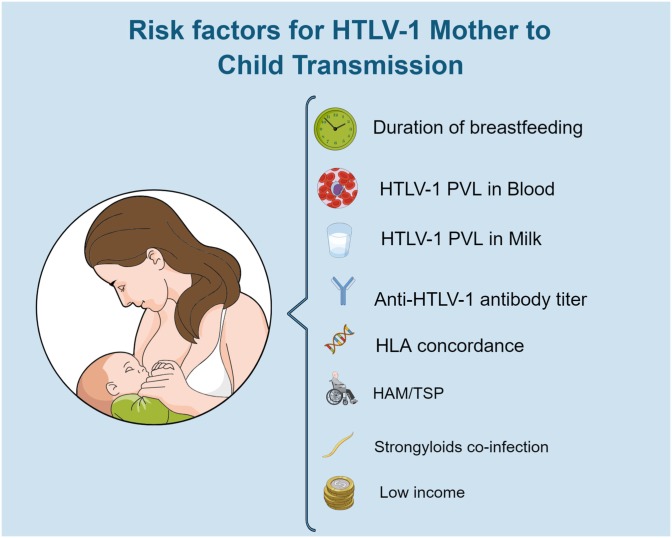
Mother-to-child transmission (MTCT) of Human T-cell lymphotropic virus type 1 (HTLV-1) causes lifelong infection. At least 5-10 million individuals worldwide are currently living with HTLV-1. Studies of regional variation are required to better understand the contribution of MTCT to the global burden of infection. Although most infected individuals remain asymptomatic ∼10% develop high morbidity, high mortality disease. Infection early in life is associated with a higher risk of disease development. Adult T-cell leukemia (ATL), which is caused by HTLV-1 and has a median survival of 8 months is linked to MTCT, indeed evidence of ATL following infection as an adult is sparse. Infective dermatitis also only occurs following neonatal infection. Whilst HTLV-1-associated myelopathy (HAM) follows sexual and iatrogenic infection approximately 30% of patients presenting with HAM/TSP acquired the infection through their mothers. HAM/TSP is a disabling neurodegenerative disease that greatly impact patient's quality of life. To date there is no cure for HTLV-1 infection other than bone marrow transplantation for ATL nor any measure to prevent HTLV-1 associated diseases in an infected individual. In this context, prevention of MTCT is expected to contribute disproportionately to reducing both the incidence of HTLV-1 and the burden of HTLV-1 associated diseases. In order to successfully avoid HTLV-1 MTCT, it is important to understand all the variables involved in this route of infection. Questions remain regarding frequency and risk factors for in utero peri-partum transmission whilst little is known about the efficacy of pre-labor cesarean section to reduce these infections. Understanding the contribution of peripartum infection to the burden of disease will be important to gauge the risk-benefit of interventions in this area. Few studies have examined the impact of HTLV-1 infection on fertility or pregnancy outcomes nor the susceptibility of the mother to infection during pregnancy and lactation. Whilst breast-feeding is strongly associated with transmission and avoidance of breast-feeding a proven intervention little is known about the mechanism of transmission from the breast milk to the infant and there have been no clinical trials of antiretroviral therapy (ARV) to prevent this route of transmission.
Keywords: HTLV-1; disease; mother-to-child transmission; outcomes; pregnancy; risk.
Figures



References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous