

Clinician Perception of a Machine Learning-Based Early Warning System Designed to Predict Severe Sepsis and Septic Shock
- PMID: 31135500
- PMCID: PMC6791738
- DOI: 10.1097/CCM.0000000000003803
Clinician Perception of a Machine Learning-Based Early Warning System Designed to Predict Severe Sepsis and Septic Shock
Abstract
Objective: To assess clinician perceptions of a machine learning-based early warning system to predict severe sepsis and septic shock (Early Warning System 2.0).
Design: Prospective observational study.
Setting: Tertiary teaching hospital in Philadelphia, PA.
Patients: Non-ICU admissions November-December 2016.
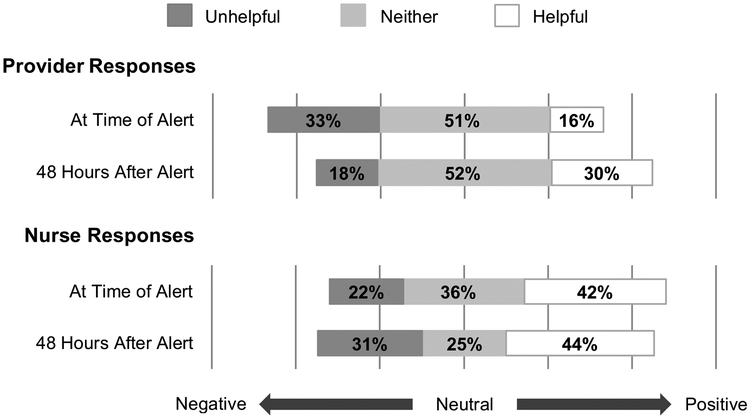
Interventions: During a 6-week study period conducted 5 months after Early Warning System 2.0 alert implementation, nurses and providers were surveyed twice about their perceptions of the alert's helpfulness and impact on care, first within 6 hours of the alert, and again 48 hours after the alert.
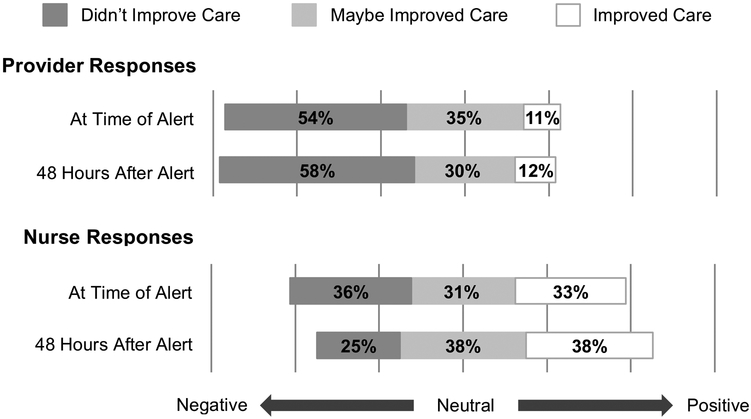
Measurements and main results: For the 362 alerts triggered, 180 nurses (50% response rate) and 107 providers (30% response rate) completed the first survey. Of these, 43 nurses (24% response rate) and 44 providers (41% response rate) completed the second survey. Few (24% nurses, 13% providers) identified new clinical findings after responding to the alert. Perceptions of the presence of sepsis at the time of alert were discrepant between nurses (13%) and providers (40%). The majority of clinicians reported no change in perception of the patient's risk for sepsis (55% nurses, 62% providers). A third of nurses (30%) but few providers (9%) reported the alert changed management. Almost half of nurses (42%) but less than a fifth of providers (16%) found the alert helpful at 6 hours.
Conclusions: In general, clinical perceptions of Early Warning System 2.0 were poor. Nurses and providers differed in their perceptions of sepsis and alert benefits. These findings highlight the challenges of achieving acceptance of predictive and machine learning-based sepsis alerts.
Figures
Comment in
-
Beware of the Magic Eight Ball in Medicine.Crit Care Med. 2019 Nov;47(11):1650-1651. doi: 10.1097/CCM.0000000000004007. Crit Care Med. 2019. PMID: 31609258 No abstract available.
References
-
- Levy MM, Rhodes A, Phillips GS, et al.: Surviving Sepsis Campaign: association between performance metrics and outcomes in a 7.5-year study. Intensive Care Med 2014; 40(11):1623–1633 - PubMed
-
- Kumar A, Roberts D, Wood KE, et al.: Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med 2006; 34(6):1589–1596 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
