

Do Skills Acquired from Training with a Wire Navigation Simulator Transfer to a Mock Operating Room Environment?
- PMID: 31135546
- PMCID: PMC6999951
- DOI: 10.1097/CORR.0000000000000799
Do Skills Acquired from Training with a Wire Navigation Simulator Transfer to a Mock Operating Room Environment?
Erratum in
-
Erratum to: Do Skills Acquired from Training with a Wire Navigation Simulator Transfer to a Mock Operating Room Environment?Clin Orthop Relat Res. 2019 Oct;477(10):2389. doi: 10.1097/CORR.0000000000000958. Clin Orthop Relat Res. 2019. PMID: 31498254 Free PMC article. No abstract available.
Abstract
Background: Skills training and simulation play an increasingly important role in orthopaedic surgical education. The intent of simulation is to improve performance in the operating room (OR), a trait known as transfer validity. No prior studies have explored how simulator-based wire navigation training can transfer to higher-level tasks. Additionally, there is a lack of knowledge on the format in which wire navigation training should be deployed.
Questions/purposes: (1) Which training methods (didactic content, deliberate practice, or proficiency-based practice) lead to the greatest improvement in performing a wire navigation task? (2) Does a resident's performance using a wire navigation simulator correlate with his or her performance on a higher-level simulation task in a mock OR involving a C-arm, a radiopaque femur model, and a large soft tissue surrogate surrounding the femur?
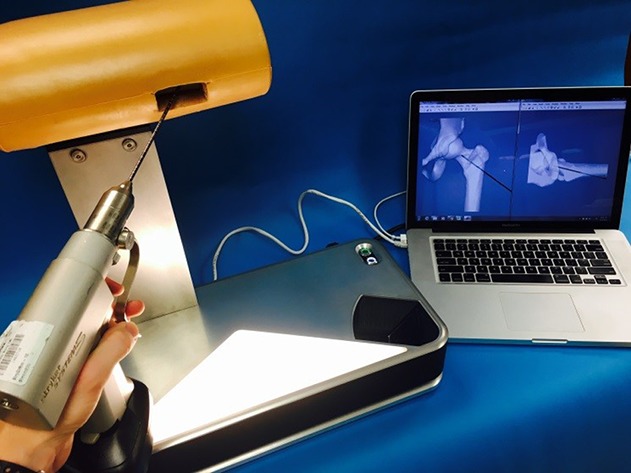
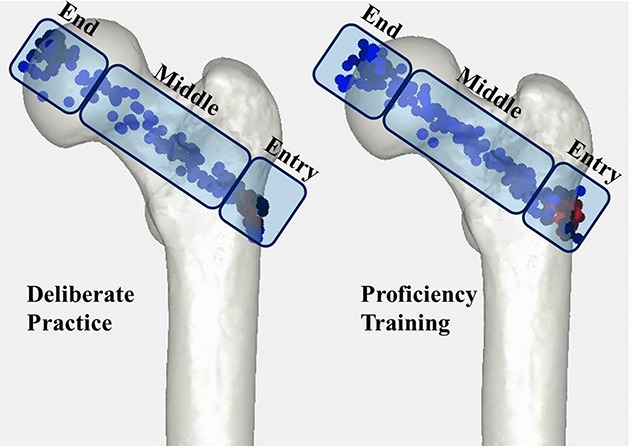
Methods: Fifty-five residents from four different medical centers participated in this study over the course of 2 years. The residents were divided into three groups: traditional training (included first-year residents from the University of Iowa, University of Minnesota, and the Mayo Clinic), deliberate practice (included first-year residents from the University of Nebraska and the University of Minnesota), and proficiency training (included first-year residents from the University of Minnesota and the Mayo Clinic). Residents in each group received a didactic introduction covering the task of placing a wire to treat an intertrochanteric fracture, and this was considered traditional training. Deliberate practice involved training on a radiation-free simulator that provided specific feedback throughout the practice sessions. Proficiency training used the same simulator to train on specific components of wire navigation, like finding the correct starting point, to proficiency before moving to assessment. The wire navigation simulator uses a camera system to track the wire and provide computer-generated fluoroscopy. After training, task performance was assessed in a mock OR. Residents from each group were assessed in the mock OR based on their use of fluoroscopy, total time, and tip-apex distance. Correlation analysis was performed to examine the relationship between resident performance on the simulator and in the mock OR.
Results: Residents in the two simulation-based training groups had a lower tip-apex distance than those in the traditional training group (didactic training tip-apex distance: 24 ± 7 mm, 95% CI, 20-27; deliberate practice tip-apex distance: 16 ± 5 mm, 95% CI, 13-19, p = 0.001; proficiency training tip-apex distance: 15 ± 4 mm, 95% CI, 13-18, p < 0.001). Residents in the proficiency training group used more images than those in the other groups (didactic training: 22 ± 12 images, p = 0.041; deliberate practice: 19 ± 8 images; p = 0.012, proficiency training: 31 ± 14 images). In the two simulation-based training groups, resident performance on the simulator, that is, tip-apex distance, image use, and overall time, was correlated with performance in the mock OR (r-square = 0.15 [p = 0.030], 0.61 [p < 0.001], and 0.43 [p < 0.001], respectively).
Conclusions: As residency programs are designing their curriculum to train wire navigation skills, emphasis should be placed on providing an environment that allows for deliberate practice with immediate feedback about their performance. Simulators such as the one presented in this study offer a safe environment for residents to learn this key skill.
Level of evidence: Level II, therapeutic study.
Conflict of interest statement
All ICMJE Conflict of Interest Forms for authors and
Figures








References
-
- Baumgaertner MR, Curtin SL, Lindskog DM, Keggi JM. The value of the tip-apex distance in predicting failure of fixation of peritrochanteric fractures of the hip. J Bone Joint Surg Am. 1995;77:1058-1064. - PubMed
-
- Bric J, Connolly M, Kastenmeier A, Goldblatt M, Gould JC. Proficiency training on a virtual reality robotic surgical skills curriculum. Surg Endosc. 2014;28:3343-3348. - PubMed
-
- Carpenter JE, Hurwitz SR, James MA, Jeffries JT, Marsh JL, Martin DF, Murray PM, Parsons BO, Pedowitz RA, Toolan BC, Heest AEV, Wongworawat MD. ABOS Surgical Skills Modules for PGY-1 Residents. Available at: https://www.abos.org/abos-surgical-skills-modules-for-pgy-1-residents.aspx. Accessed May 20, 2018.
-
- Cecil J, Gupta A, Pirela-Cruz M. An advanced simulator for orthopedic surgical training. Int J Comput Assist Radiol Surg. 2018;13:305-319. - PubMed
-
- Centers for Disease Control and Prevention. Hip fractures among older adults. Available at: https://www.cdc.gov/homeandrecreationalsafety/falls/adulthipfx.html. Accessed May 20, 2018.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
