

Change in Patient Outcomes After Augmenting a Low-level Implementation Strategy in Community Practices That Are Slow to Adopt a Collaborative Chronic Care Model: A Cluster Randomized Implementation Trial
- PMID: 31135692
- PMCID: PMC6684247
- DOI: 10.1097/MLR.0000000000001138
Change in Patient Outcomes After Augmenting a Low-level Implementation Strategy in Community Practices That Are Slow to Adopt a Collaborative Chronic Care Model: A Cluster Randomized Implementation Trial
Abstract
Background: Implementation strategies are essential for promoting the uptake of evidence-based practices and for patients to receive optimal care. Yet strategies differ substantially in their intensity and feasibility. Lower-intensity strategies (eg, training and technical support) are commonly used but may be insufficient for all clinics. Limited research has examined the comparative effectiveness of augmentations to low-level implementation strategies for nonresponding clinics.
Objectives: To compare 2 augmentation strategies for improving uptake of an evidence-based collaborative chronic care model (CCM) on 18-month outcomes for patients with depression at community-based clinics nonresponsive to lower-level implementation support.
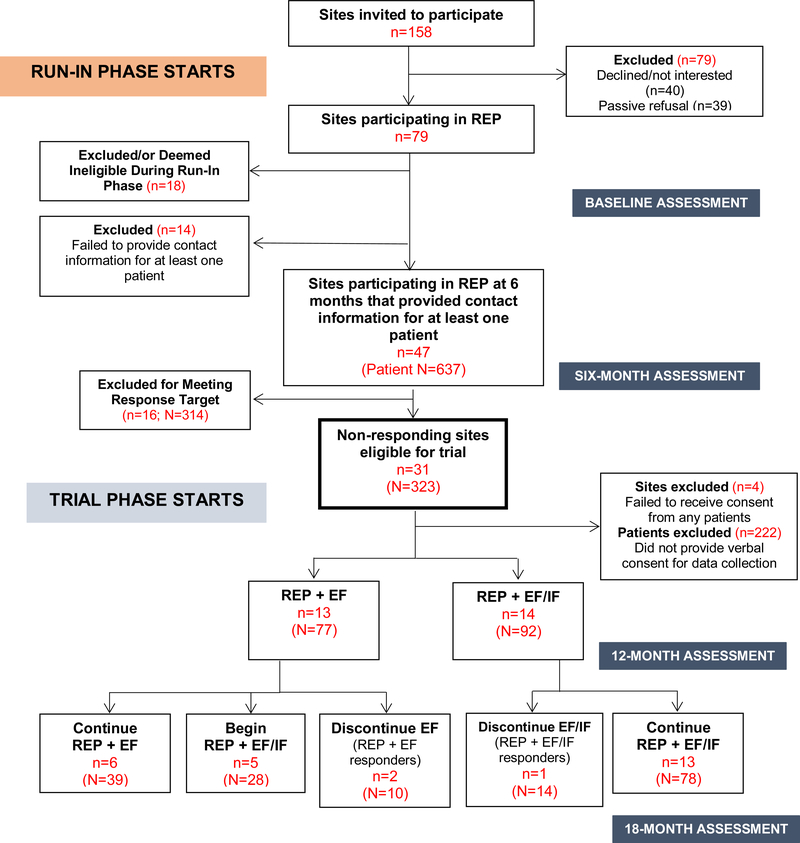
Research design: Providers initially received support using a low-level implementation strategy, Replicating Effective Programs (REP). After 6 months, nonresponsive clinics were randomized to add either external facilitation (REP+EF) or external and internal facilitation (REP+EF/IF).
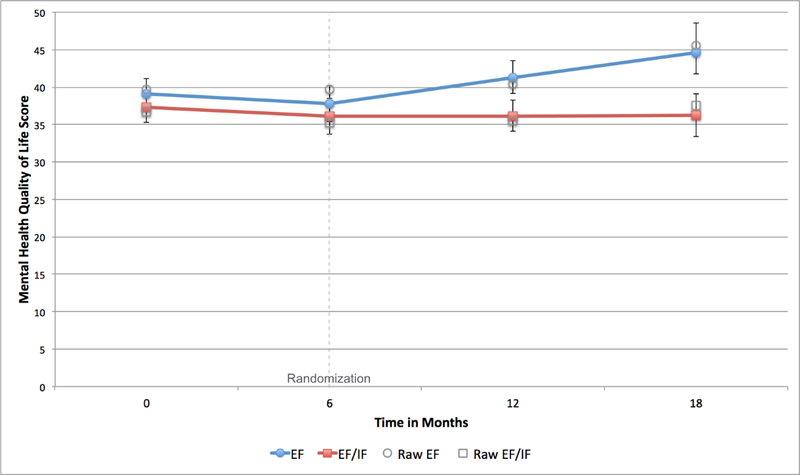
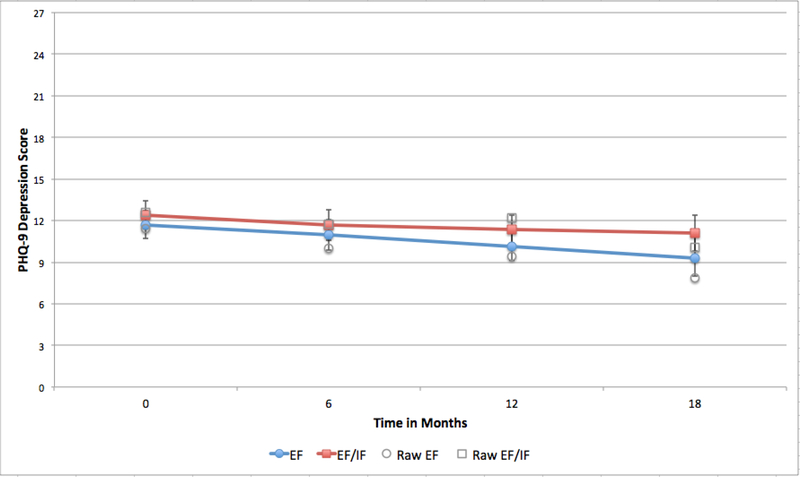
Measures: The primary outcome was patient 12-item short form survey (SF-12) mental health score at month 18. Secondary outcomes were patient health questionnaire (PHQ-9) depression score at month 18 and receipt of the CCM during months 6 through 18.
Results: Twenty-seven clinics were nonresponsive after 6 months of REP. Thirteen clinics (N=77 patients) were randomized to REP+EF and 14 (N=92) to REP+EF/IF. At 18 months, patients in the REP+EF/IF arm had worse SF-12 [diff, 8.38; 95% confidence interval (CI), 3.59-13.18] and PHQ-9 scores (diff, 1.82; 95% CI, -0.14 to 3.79), and lower odds of CCM receipt (odds ratio, 0.67; 95% CI, 0.30-1.49) than REP+EF patients.
Conclusions: Patients at sites receiving the more intensive REP+EF/IF saw less improvement in mood symptoms at 18 months than those receiving REP+EF and were no more likely to receive the CCM. For community-based clinics, EF augmentation may be more feasible than EF/IF for implementing CCMs.
Trial registration: ClinicalTrials.gov NCT02151331.
Figures
References
-
- Woltmann E, Grogan-Kaylor A, Perron B, Georges H, Kilbourne AM, Bauer MS. Comparative effectiveness of collaborative chronic care models for mental health conditions across primary, specialty, and behavioral health care settings: systematic review and meta-analysis. American Journal of Psychiatry. 2012;169(8):790–804. - PubMed
-
- Kilbourne AM, Li D, Lai Z, Waxmonsky J, Ketter T. Pilot randomized trial of a cross‐diagnosis collaborative care program for patients with mood disorders. Depression and anxiety. 2013;30(2):116–122. - PubMed
-
- Roy-Byrne PP, Sherbourne CD, Craske MG, et al. Moving treatment research from clinical trials to the real world. Psychiatric Services. 2003;54(3):327–332. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
