

Parafoveal thinning of inner retina is associated with visual dysfunction in Lewy body diseases
- PMID: 31136022
- PMCID: PMC6790692
- DOI: 10.1002/mds.27728
Parafoveal thinning of inner retina is associated with visual dysfunction in Lewy body diseases
Abstract
Background: Retinal optical coherence tomography findings in Lewy body diseases and their implications for visual outcomes remain controversial. We investigated whether region-specific thickness analysis of retinal layers could improve the detection of macular atrophy and unravel its association with visual disability in Parkinson's disease.
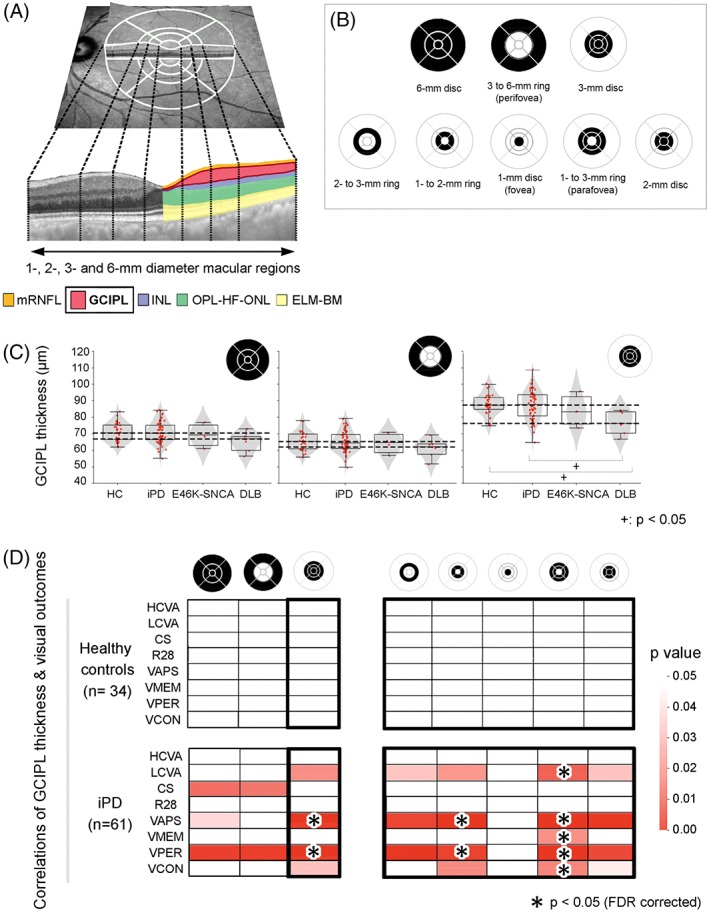
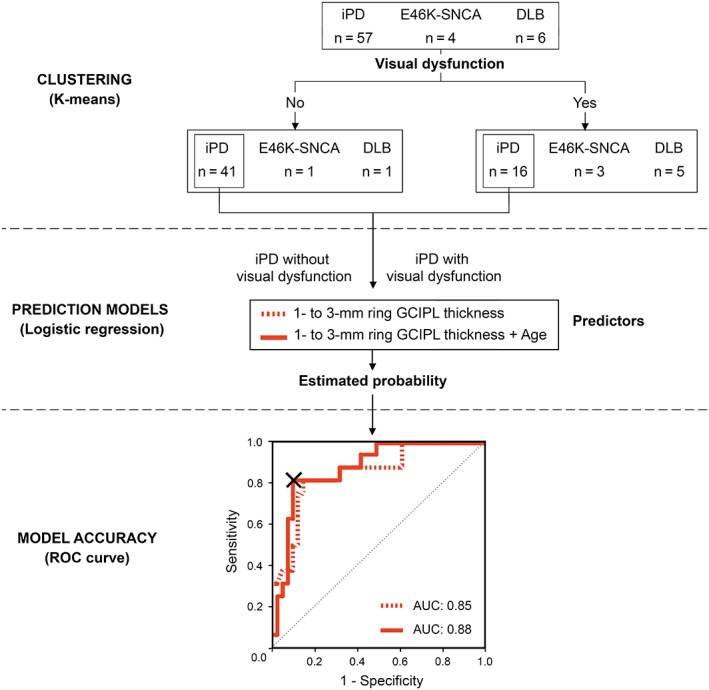
Methods: Patients with idiopathic Parkinson's disease (n = 63), dementia with Lewy bodies (n = 8), and E46K mutation carriers in the α-synuclein gene (E46K-SNCA) (n = 4) and 34 controls underwent Spectralis optical coherence tomography macular scans and a comprehensive battery of visual function and cognition tests. We computed mean retinal layer thicknesses of both eyes within 1-, 2-, 3-, and 6-mm diameter macular discs and in concentric parafoveal (1- to 2-mm, 2- to 3-mm, 1- to 3-mm) and perifoveal (3- to 6-mm) rings. Group differences in imaging parameters and their relationship with visual outcomes were analyzed. A multivariate logistic model was developed to predict visual impairment from optical coherence tomography measurements in Parkinson's disease, and cutoff values were determined with receiver operating characteristic analysis.
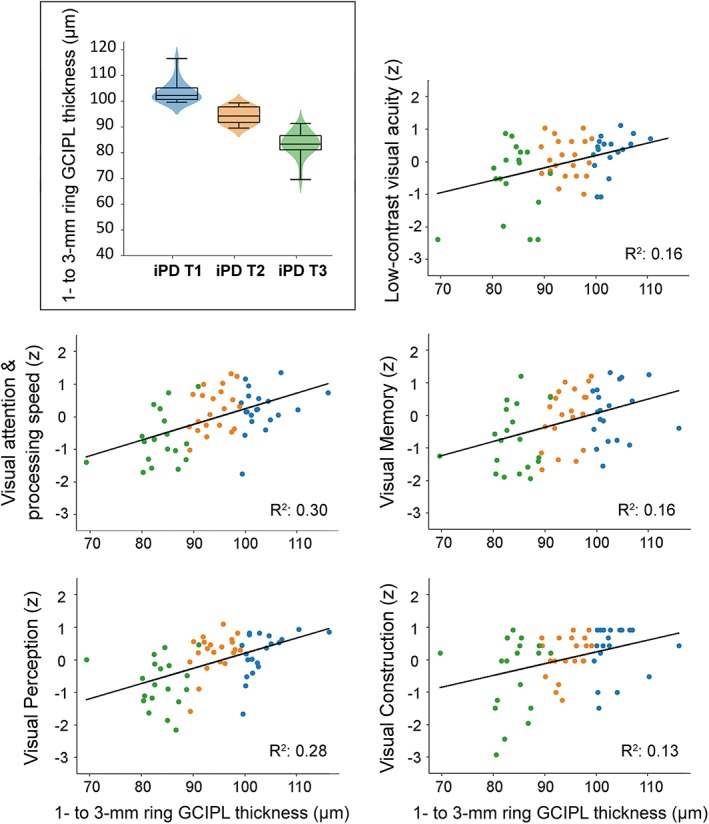
Results: When compared with controls, patients with dementia with Lewy bodies had significant thinning of the ganglion cell-inner plexiform layer complex within the central 3-mm disc mainly because of differences in 1- to 3-mm parafoveal thickness. This parameter was strongly correlated in patients, but not in controls, with low contrast visual acuity and visual cognition outcomes (P < .05, False Discovery Rate), achieving 88% of accuracy in predicting visual impairment in Parkinson's disease.
Conclusion: Our findings support that parafoveal thinning of ganglion cell-inner plexiform complex is a sensitive and clinically relevant imaging biomarker for Lewy body diseases, specifically for Parkinson's disease. © 2019 The Authors. Movement Disorders published by Wiley Periodicals, Inc. on behalf of International Parkinson and Movement Disorder Society.
Keywords: Parkinson's disease; dementia with Lewy bodies; macula; optical coherence tomography; visual dysfunction.
© 2019 The Authors. Movement Disorders published by Wiley Periodicals, Inc. on behalf of International Parkinson and Movement Disorder Society.
Figures
Comment in
-
Clinical and cognitive correlates of selective regional retinal thinning in dementia with lewy bodies.Mov Disord. 2019 Oct;34(10):1582-1583. doi: 10.1002/mds.27851. Mov Disord. 2019. PMID: 31769090 No abstract available.
-
Reply to: Clinical and cognitive correlates of selective regional retina thinning in dementia with lewy bodies.Mov Disord. 2019 Oct;34(10):1584. doi: 10.1002/mds.27850. Mov Disord. 2019. PMID: 31769091 No abstract available.
References
-
- Zarranz JJ, Alegre J, Gomez‐Esteban JC, et al. The new mutation, E46K, of alpha‐synuclein causes Parkinson and Lewy body dementia. Ann Neurol 2004;55(2):164‐173. - PubMed
-
- Schapira AHV, Chaudhuri KR, Jenner P. Non‐motor features of Parkinson disease. Nat Rev Neurosci 2017;18(7):435‐450. - PubMed
-
- Armstrong RA. Visual dysfunction in Parkinson's disease. Int Rev Neurobiol 2017;134:921‐946. - PubMed
-
- Williams‐Gray CH, Foltynie T, Brayne CE, Robbins TW, Barker RA. Evolution of cognitive dysfunction in an incident Parkinson's disease cohort. Brain 2007;130(Pt 7):1787‐1798. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
