

Conversion of Hemiarthroplasty to THA Carries an Increased Risk of Reoperation Compared With Primary and Revision THA
- PMID: 31136440
- PMCID: PMC6554100
- DOI: 10.1097/CORR.0000000000000702
Conversion of Hemiarthroplasty to THA Carries an Increased Risk of Reoperation Compared With Primary and Revision THA
Abstract
Background: There is limited information on the complications and costs of conversion THA after hemiarthroplasty for femoral neck fractures. Previous studies have found that patients undergoing conversion THA experience higher risk complications, but it has been difficult to quantify the risk because of small sample sizes and a lack of comparison groups. Therefore, we compared the complications of patients undergoing conversion THA with strictly matched patients undergoing primary and revision THA.
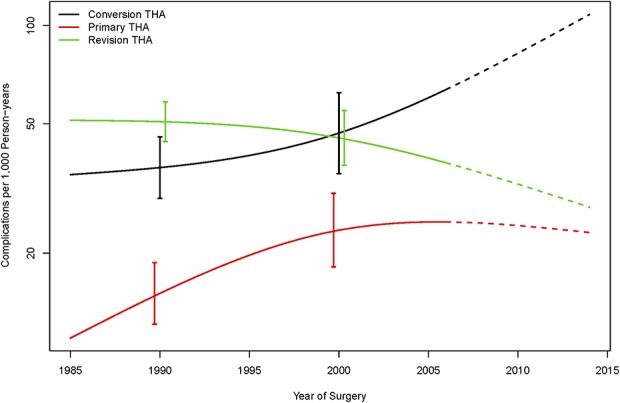
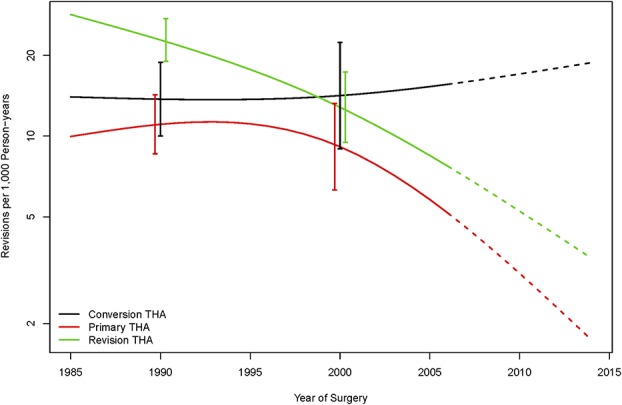
Questions/purposes: (1) What are the risks of complications, dislocations, reoperations, revisions and periprosthetic fractures after conversion THA compared with primary and revision THA and how has this effect changed over time? (2) What are the length of hospital stay and hospital costs for conversion THA, primary THA, and revision THA?
Methods: Using a longitudinally maintained total joint registry, we identified 389 patients who were treated with conversion THA after hemiarthroplasty for femoral neck fractures between 1985 and 2014. The conversion THA cohort was 1:2 matched on age, sex, and year of surgery to 778 patients undergoing primary THA and 778 patients undergoing revision THA. The proportion of patients having at least 5-year followup was 73% in those who underwent conversion THA, 77% in those who underwent primary THA, and 76% in those who underwent revision THA. We observed a significant calendar year effect, and therefore, compared the three groups across two separate time periods: 1985 to 1999 and 2000 to 2014. We ascertained complications, dislocations, reoperations, revisions and periprosthetic fractures from the total joint registry. Cost analysis was performed using a bottom-up, microcosting methodology for procedures between 2003 and 2014.
Results: Patients who converted to THA between 1985 and 1999 had a higher risk of complications (hazard ratio [HR], 2.3; 95% confidence interval [CI], 1.7-3.1; p < 0.001), dislocations (HR, 2.3; 95% CI, 1.3-4.2; p = 0.007), reoperations (HR, 1.7; 95% CI, 1.2-2.5, p = 0.005), and periprosthetic fractures (HR, 3.8; 95% CI, 2.2-6.6; p < 0.001) compared with primary THA. However, conversion THAs during the 1985 to 1999 time period had a lower risk of reoperations (HR, 0.7; 95% CI, 0.5-1.0; p = 0.037), revisions (HR, 0.6; 95% CI, 0.5-0.9; p = 0.014), and periprosthetic fractures (HR, 0.6; 95% CI, 0.4-0.9; p = 0.007) compared with revision THA. The risk differences across the three groups were more pronounced after 2000, particularly when comparing conversion THA patients with revision THA. Conversion THA patients had a higher risk of reoperations (HR, 1.9; 95% CI, 1.0-3.4; p = 0.041) and periprosthetic fractures (HR, 1.7; 95% CI, 1.0-2.9; p = 0.036) compared with revision THA, but there were no differences in the complication risk (HR, 1.4; 95% CI, 0.9-2.1; p = 0.120), dislocations (HR, 1.5; 95% CI, 0.7-3.2; p = 0.274), and revisions (HR, 1.4; 95% CI, 0.7-3.0; p = 0.373). Length of stay for conversion THA was longer than primary THA (4.7 versus 4.0 days; p = 0.012), but there was no difference compared with revision THA (4.7 versus 4.5 days; p = 0.484). Similarly, total inpatient costs for conversion THA were higher than primary THA (USD 22,662 versus USD 18,694; p < 0.001), but there was no difference compared with revision THA (USD 22,662 versus USD 22,071; p = 0.564).
Conclusions: Over the 30 years of the study, conversion THA has remained a higher risk procedure in terms of reoperation compared with primary THA, and over time, it also has become higher risk compared with revision THA. Surgeons should approach conversion THA as a challenging procedure, and patients undergoing this procedure should be counseled about the elevated risks. Furthermore, hospitals should seek appropriate reimbursement for these cases.
Level of evidence: Level III, therapeutic study.
Conflict of interest statement
All ICMJE Conflict of Interest Forms for authors and
Figures
Comment in
-
CORR Insights®: Conversion of Hemiarthroplasty to THA Carries an Increased Risk of Reoperation Compared With Primary and Revision THA.Clin Orthop Relat Res. 2019 Jun;477(6):1400-1401. doi: 10.1097/CORR.0000000000000779. Clin Orthop Relat Res. 2019. PMID: 31136441 Free PMC article. No abstract available.
References
-
- Abrahamsen B, van Staa T, Ariely R, Olson M, Cooper C. Excess mortality following hip fracture: a systematic epidemiological review. Osteoporos Int. 2009;20:1633-1650. - PubMed
-
- American Joint Replacement Registry. American Joint Replacement Registry Annual Report 2016, 15, 2016. Available at: http://www.ajrr.net/publications-data/annual-reports. Accessed December, 5, 2018.
-
- Baghoolizadeh M, Schwarzkopf R. The Lawrence D. Dorr Surgical Techniques & Technologies Award: Conversion total hip arthroplasty: Is it a primary or revision hip arthroplasty. J Arthroplasty. 2016;31:16-21. - PubMed
-
- Burgers PT, Van Geene AR, Van den Bekerom MP, Van Lieshout EM, Blom B, Aleem IS, Bhandari M, Poolman RW. Total hip arthroplasty versus hemiarthroplasty for displaced femoral neck fractures in the healthy elderly: a meta-analysis and systematic review of randomized trials. Int Orthop. 2012;36:1549-1560. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
