

Risk Factors for Rapid Progression From Acute Recurrent to Chronic Pancreatitis in Children: Report From INSPPIRE
- PMID: 31136562
- PMCID: PMC6699635
- DOI: 10.1097/MPG.0000000000002405
Risk Factors for Rapid Progression From Acute Recurrent to Chronic Pancreatitis in Children: Report From INSPPIRE
Abstract
Objective: The aim of the study was to determine the rate of progression from acute recurrent pancreatitis (ARP) to chronic pancreatitis (CP) in children and assess risk factors.
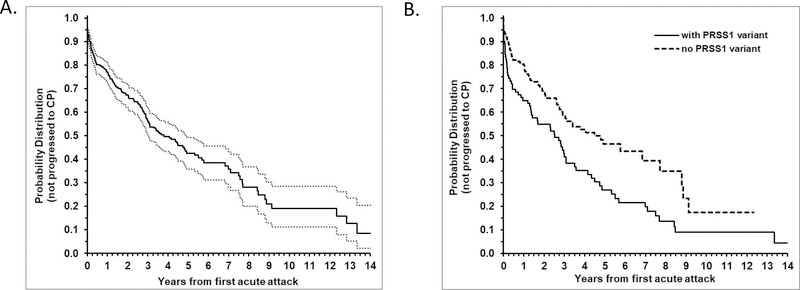
Study design: Data were collected from the INternational Study group of Pediatric Pancreatitis: In search for a cuRE (INSPPIRE) cohort. Kaplan-Meier curves were constructed to calculate duration of progression from initial attack of acute pancreatitis (AP) to CP. Log-rank test was used to compare survival (nonprogression) probability distribution between groups. Cox proportional hazard regression models were fitted to obtain hazard ratio (with 95% confidence interval [CI]) of progression for each risk variable.
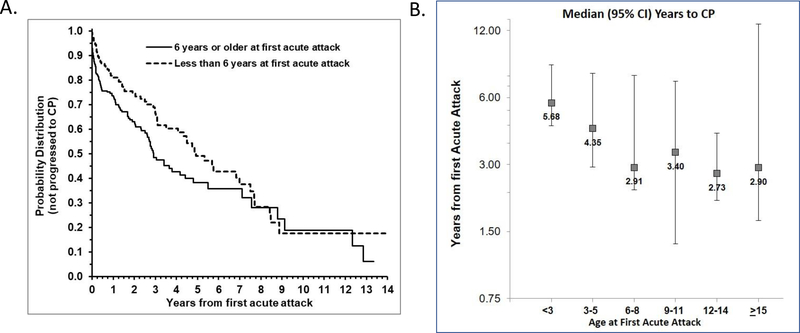
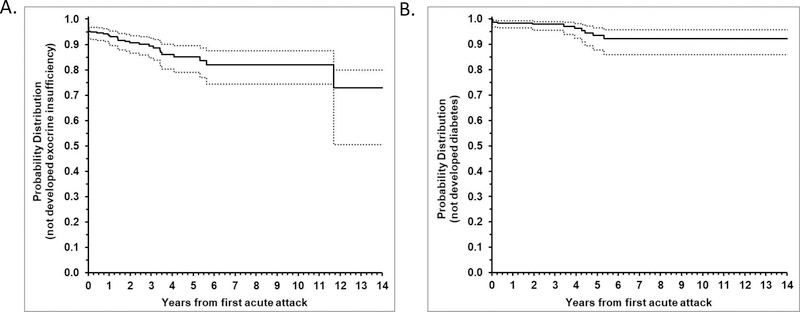
Results: Of 442 children, 251 had ARP and 191 had CP. The median time of progression from initial attack of AP to CP was 3.79 years. The progression was faster in those ages 6 years or older at the first episode of AP compared to those younger than 6 years (median time to CP: 2.91 vs 4.92 years; P = 0.01). Children with pathogenic PRSS1 variants progressed more rapidly to CP compared to children without PRSS1 variants (median time to CP: 2.52 vs 4.48 years; P = 0.003). Within 6 years after the initial AP attack, cumulative proportion with exocrine pancreatic insufficiency was 18.0% (95% CI: 12.4%, 25.6%); diabetes mellitus was 7.7% (95% CI: 4.2%, 14.1%).
Conclusions: Children with ARP rapidly progress to CP, exocrine pancreatic insufficiency, and diabetes. The progression to CP is faster in children who were 6 years or older at the first episode of AP or with pathogenic PRSS1 variants. The factors that affect the aggressive disease course in childhood warrant further investigation.
Figures
References
-
- Lowenfels AB, Maisonneuve P, Cavallini G, et al. Pancreatitis and the risk of pancreatic cancer. International Pancreatitis Study Group. N Engl J Med 1993;328:1433–7. - PubMed
-
- Whitcomb DC, Gorry MC, Preston RA, et al. Hereditary pancreatitis is caused by a mutation in the cationic trypsinogen gene. Nat Genet 1996;14:141–5. - PubMed
