

New insights into the prevalence of depressive symptoms and depression in rheumatoid arthritis - Implications from the prospective multicenter VADERA II study
- PMID: 31136632
- PMCID: PMC6538160
- DOI: 10.1371/journal.pone.0217412
New insights into the prevalence of depressive symptoms and depression in rheumatoid arthritis - Implications from the prospective multicenter VADERA II study
Abstract
Objectives: To investigate the prevalence of depressive symptoms in rheumatoid arthritis (RA) patients using two previously validated questionnaires in a large patient sample, and to evaluate depressive symptoms in the context of clinical characteristics (e.g. remission of disease) and patient-reported impact of disease.
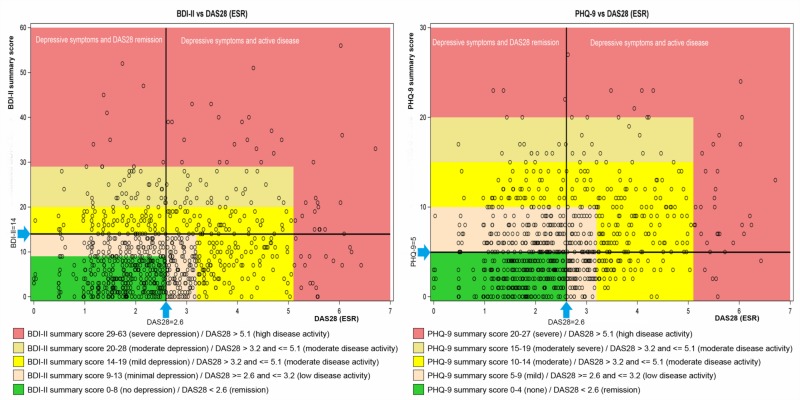
Methods: In this cross-sectional study, the previously validated Patient Health Questionnaire (PHQ-9) and Beck-Depression Inventory II (BDI-II) were used to assess the extent of depressive symptoms in RA patients. Demographic background, RA disease activity score (DAS28), RA impact of disease (RAID) score, comorbidities, anti-rheumatic therapy and antidepressive treatment, were recorded. Cut-off values for depressive symptomatology were PHQ-9 ≥5 or BDI-II ≥14 for mild depressive symptoms or worse and PHQ-9 ≥ 10 or BDI-II ≥ 20 for moderate depressive symptoms or worse. Prevalence of depressive symptomatology was derived by frequency analysis while factors independently associated with depressive symptomatology were investigated by using multiple logistic regression analyses. Ethics committee approval was obtained, and all patients provided written informed consent before participation.
Results: In 1004 RA-patients (75.1% female, mean±SD age: 61.0±12.9 years, mean disease duration: 12.2±9.9 years, DAS28 (ESR): 2.5±1.2), the prevalence of depressive symptoms was 55.4% (mild or worse) and 22.8% (moderate or worse). Characteristics independently associated with depressive symptomatology were: age <60 years (OR = 1.78), RAID score >2 (OR = 10.54) and presence of chronic pain (OR = 3.25). Of patients classified as having depressive symptoms, only 11.7% were receiving anti-depressive therapy.
Conclusions: Mild and moderate depressive symptoms were common in RA patients according to validated tools. In routine clinical practice, screening for depression with corresponding follow-up procedures is as relevant as incorporating these results with patient-reported outcomes (e.g. symptom state), because the mere assessment of clinical disease activity does not sufficiently reflect the prevalence of depressive symptoms.
Clinical trial registration number: This study is registered in the Deutsches Register Klinischer Studien (DRKS00003231) and ClinicalTrials.gov (NCT02485483).
Conflict of interest statement
This work was funded by Roche Pharma AG and Chugai Pharma Europe Ltd. Besides Dr. Flacke’s and Dr. Hofmann’s support at the study conception phase and the review of the statistical analysis plan by an independent statistician on behalf of Roche, Roche Pharma AG and Chugai Pharma Europe Ltd. had no further direct role in the collection, analysis, or interpretation of the data. AMS Advanced Medical Services GmbH (Mannheim, Germany) was involved in the study as a contract research organization on behalf of the study sponsors conducting the data analysis in collaboration with the scientific project leaders and supporting manuscript preparation. Drs. Englbrecht, Alten, Aringer, Baerwald, Burkhardt, Fliedner, Kleinert, Kneitz, Krueger, Schett, Schmalzing, Tausche, Tony, and Wendler received grants, honoraria, consulting fees, and/or speaking fees (less than $10,000 each) from Roche Pharma AG and Chugai Pharma Europe Ltd. Dr. Englbrecht has received speaker’s fees, compensation for consultancies or board memberships from: AbbVie, Celgene, Lilly, Mundipharma, Novartis, Pfizer, UCB. Dr. Aringer reports AbbVie, Astra Zeneca, Boehringer Ingelheim, Chugai, GSK, HEXAL, Lilly, MSD, Novartis, Pfizer, Roche, Sandoz and Sanofi advisory boards, speaking fees and/or congress support. Dr. Baewald has received travel grants and speaking honoraria or is on advisory boards for Abbvie, Amgen, Biogen, BMS, Janssen, Lilly, MSD, Pfizer and UCB. Dr. Fliedner is on advisory boards for Abbvie, BMS, and Pfizer and has participated in meetings for UBC, Lilly, and Pfizer. Dr. Schett’s work was supported by the Metarthros program of the BMBF. Dr. Schmalzing has received speaker’s fees, travel grants, research funding, or compensation for consultancies or board memberships from: Abbvie, Actelion, BMS, Celgene, Genzyme, Hexal/Sandoz, Janssen‐Cilag, MSD, Novartis, Pfizer, Sanofi Pasteur, Shire (Baxalta), and UCB. Dr. Wendler is a member of Roche and Chugai advisory boards. Dr. Kneitz has received speaker’s fees, compensation for consultancies or board memberships of: AbbVie, Berlin Chemie, BMS, Celgene, Janssen, Lilly, MSD, Novartis, Pfizer, Sanofi, and UCB. Dr. Eby received fees from Roche Pharma AG for manuscript preparation and statistical analysis. Dr. Flacke is an employee of Roche Pharma AG. and Dr. Hofmann is an employee of Chugai Pharma Europe Ltd. Editorial assistance for this manuscript was provided by Physicians World Europe (Mannheim, Germany), sponsored by Roche Pharma AG. Funding by corporate entities does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
