

18F-FDG PET/CT and Urothelial Carcinoma: Impact on Management and Prognosis-A Multicenter Retrospective Study
- PMID: 31137599
- PMCID: PMC6562413
- DOI: 10.3390/cancers11050700
18F-FDG PET/CT and Urothelial Carcinoma: Impact on Management and Prognosis-A Multicenter Retrospective Study
Abstract
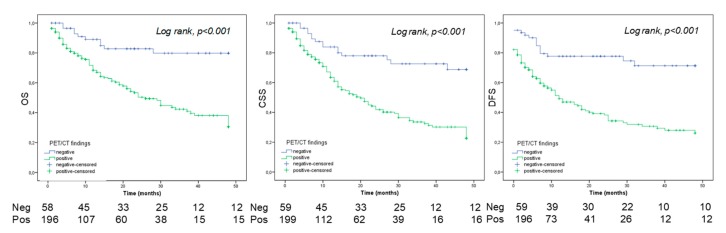
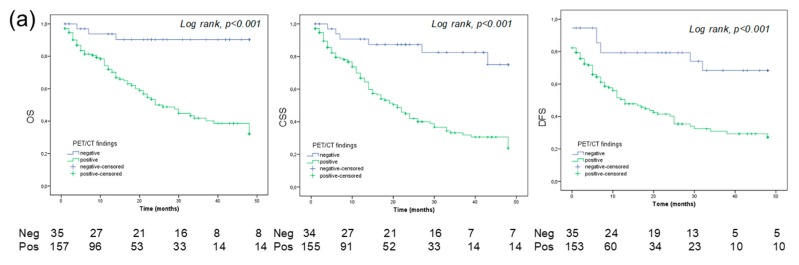
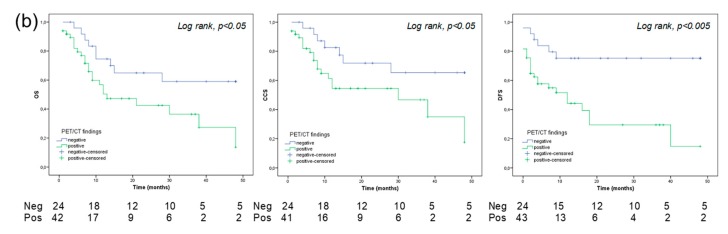
Objectives: To evaluate the ability of 18F-labeled fluoro-2-deoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT) to predict survivorship of patients with bladder cancer (BC) and/or upper urinary tract carcinoma (UUTC). Materials: Data from patients who underwent FDG PET/CT for suspicion of recurrent urothelial carcinoma (UC) between 2007 and 2015 were retrospectively collected in a multicenter study. Disease management after the introduction of FDG PET/CT in the diagnostic algorithm was assessed in all patients. Kaplan-Meier and log-rank analysis were computed for survival assessment. A Cox regression analysis was used to identify predictors of recurrence and death, for BC, UUTC, and concomitant BC and UUTC. Results: Data from 286 patients were collected. Of these, 212 had a history of BC, 38 of UUTC and 36 of concomitant BC and UUTC. Patient management was changed in 114/286 (40%) UC patients with the inclusion of FDG PET/CT, particularly in those with BC, reaching 74% (n = 90/122). After a mean follow-up period of 21 months (Interquartile range: 4-28 mo.), 136 patients (47.4%) had recurrence/progression of disease. Moreover, 131 subjects (45.6%) died. At Kaplan-Meier analyses, patients with BC and positive PET/CT had a worse overall survival than those with a negative scan (log-rank < 0.001). Furthermore, a negative PET/CT scan was associated with a lower recurrence rate than a positive examination, independently from the primary tumor site. At multivariate analysis, in patients with BC and UUTC, a positive FDG PET/CT resulted an independent predictor of disease-free and overall survival (p < 0,01). Conclusions: FDG PET/CT has the potential to change patient management, particularly for patients with BC. Furthermore, it can be considered a valid survival prediction tool after primary treatment in patients with recurrent UC. However, a firm recommendation cannot be made yet. Further prospective studies are necessary to confirm our findings.
Keywords: PET/CT; bladder cancer; survival; upper tract urothelial carcinoma; urothelial carcinoma.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Jeldres C., Sun M., Isbarn H., Lughezzani G., Budaus L., Alasker A., Shariat S.F., Lattouf J.B., Widmer H., Pharand D., et al. A population-based assessment of perioperative mortality after nephroureterectomy for upper-tract urothelial carcinoma. Urology. 2010;75:315–320. doi: 10.1016/j.urology.2009.10.004. - DOI - PubMed
LinkOut - more resources
Full Text Sources
