

Malignancy Risk and Hormonal Activity of Adrenal Incidentalomas in a Large Cohort of Patients from a Single Tertiary Reference Center
- PMID: 31137898
- PMCID: PMC6571894
- DOI: 10.3390/ijerph16101872
Malignancy Risk and Hormonal Activity of Adrenal Incidentalomas in a Large Cohort of Patients from a Single Tertiary Reference Center
Abstract
Background: A rise in adrenal incidentalomas (AIs) detection has been observed recently. Even though AIs are detected in asymptomatic patients, thorough assessment may reveal hormonal and metabolic abnormalities or malignant character.
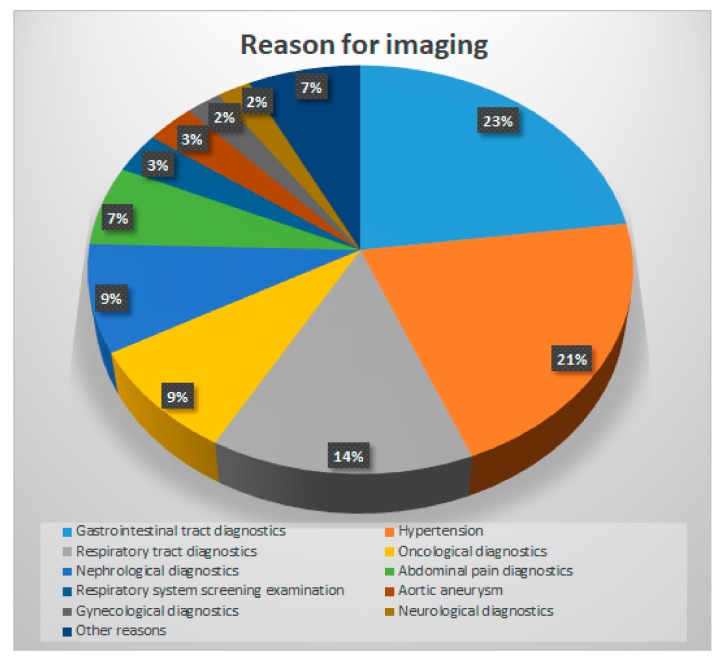
Methods: Medical records of 2005 patients (1301 women, 704 men) with 2498 tumors aged 61 ± 11.3 (18-93) years, who had been hospitalized due to AI diagnosis, were reviewed. Patients underwent clinical examination, adrenal CT and hormonal assessment. In patients subjected to adrenalectomy, histopathological character of AI was confirmed.
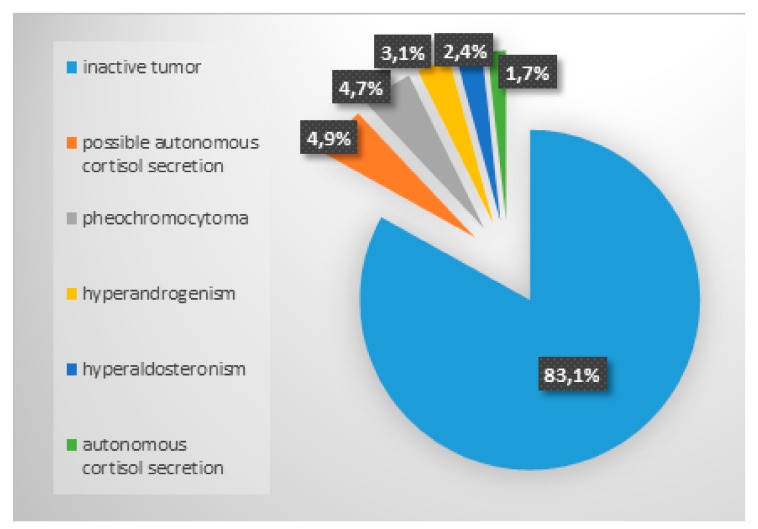
Results: AIs most frequently occurred in patients in their 7th decade of life. Hypertension was present in 76.6%, glucose metabolism disorders in 41.3%, and hypercholesterolemia in 60.1% of patients. Lipid-rich adenomas (83.2%) and hormonally inactive tumors (83.1%) predominated. Autonomous cortisol secretion was present or suspected in 6.6%, pheochromocytoma in 4.7%, hyperandrogenism in 3.1%, and primary hyperaldosteronism in 2.4% of patients. The risk of malignancy increased in patients with tumors >6 cm was 37.7%. The logistic regression analysis revealed that the strongest predictor of hormonal activity of AIs was lipid-poor picture on CT scan (OR 7.072; CI 5.118-9.771), while the most important factor increasing the risk of malignancy was lipid-poor adenoma or non-adenoma on CT scan (OR 4.843; CI 1.697-13.819). Final histopathology was available for 214 tumors; 106 adrenocortical adenomas, 46 pheochromocytomas, and 18 adrenocortical carcinomas were diagnosed.
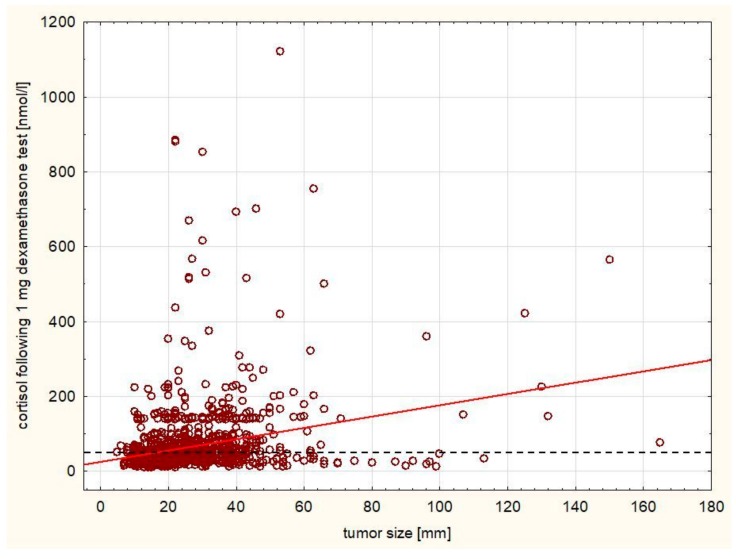
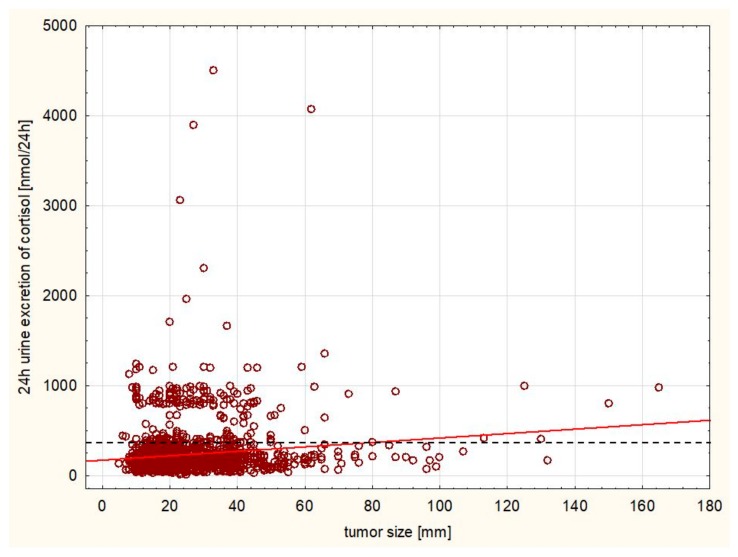
Conclusion: Most AIs are hormonally inactive adenomas. The most frequent hormonal manifestation of AI is subclinical hypercortisolemia. Presence of AI is often accompanied by features of metabolic syndrome. The tumor density on CT scan picture may be predictive of both hormonal activity and the risk of malignancy. Tumors of all sizes may exhibit hormonal activity, while the risk of malignancy significantly increases with the size above 6 cm.
Keywords: adrenal cancer; adrenal incidentaloma; adrenal tumor; autonomous cortisol secretion; pheochromocytoma; primary hyperaldosteronism.
Conflict of interest statement
Authors have no conflict of interest to disclose regarding this manuscript.
Figures
References
-
- Geelhoed G.W., Druy E.M. Management of the adrenal “incidentaloma”. Surgery. 1982;92:866–874. - PubMed
-
- Griffing G.T. A-I-D-S: The new endocrine epidemic. J. Clin. Endocrinol. Metab. 1994;79:1530–1531. - PubMed
-
- Cyranska-Chyrek E., Grzymislawska M., Ruchala M. Diagnostic pitfalls of adrenal incidentaloma. Endokrynol. Pol. 2017;68:360–377. - PubMed
-
- Grumbach M.M., Biller B.M., Braunstein G.D., Campbell K.K., Carney J.A., Godley P.A., Harris E.L., Lee J.K., Oertel Y.C., Posner M.C., et al. Management of the clinically inapparent adrenal mass (“incidentaloma”) Ann. Intern. Med. 2003;138:424–429. doi: 10.7326/0003-4819-138-5-200303040-00013. - DOI - PubMed
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
