

It's not you, it's the design - common problems with patient monitoring reported by anesthesiologists: a mixed qualitative and quantitative study
- PMID: 31138143
- PMCID: PMC6540409
- DOI: 10.1186/s12871-019-0757-z
It's not you, it's the design - common problems with patient monitoring reported by anesthesiologists: a mixed qualitative and quantitative study
Abstract
Background: Patient monitoring is critical for perioperative patient safety as anesthesiologists routinely make crucial therapeutic decisions from the information displayed on patient monitors. Previous research has shown that today's patient monitoring has room for improvement in areas such as information overload and alarm fatigue. The rationale of this study was to learn more about the problems anesthesiologists face in patient monitoring and to derive improvement suggestions for next-generation patient monitors.
Methods: We conducted a two-center qualitative/quantitative study. Initially, we interviewed 120 anesthesiologists (physicians and nurses) about the topic: common problems with patient monitoring in your daily work. Through deductive and inductive coding, we identified major topics and sub themes from the interviews. In a second step, a field survey, a separate group of 25 anesthesiologists rated their agree- or disagreement with central statements created for all identified major topics.
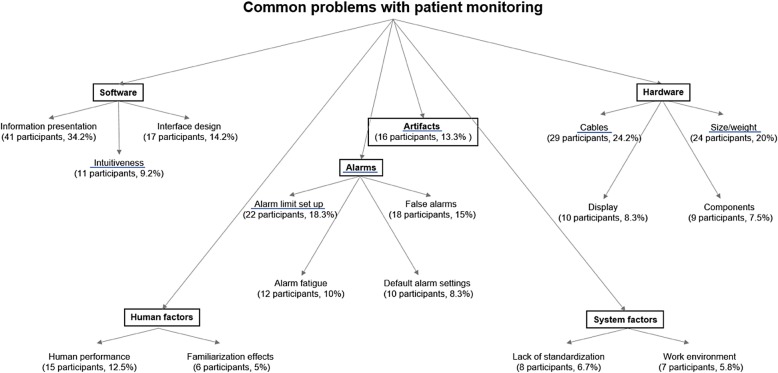
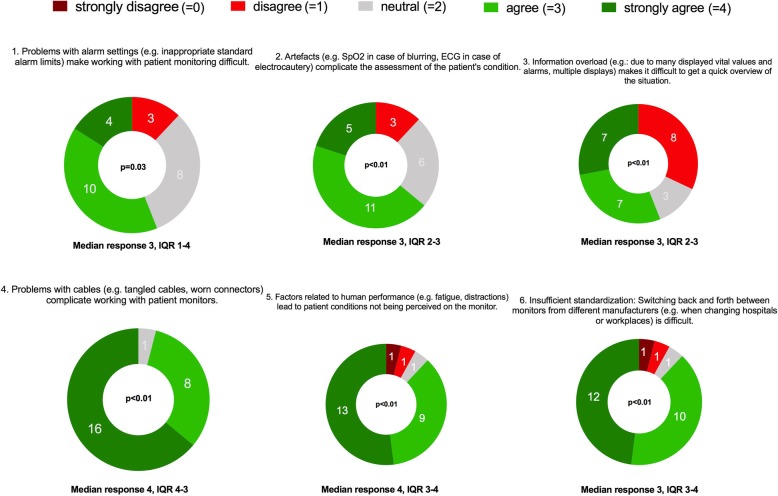
Results: We identified the following six main topics: 1. "Alarms," 2. "Artifacts," 3. "Software," 4. "Hardware," 5. "Human Factors," 6. "System Factors," and 17 sub themes. The central statements rated for the major topics were: 1. "problems with alarm settings complicate patient monitoring." (56% agreed) 2. "artifacts complicate the assessment of the situation." (64% agreed) 3. "information overload makes it difficult to get an overview quickly." (56% agreed) 4. "problems with cables complicate working with patient monitors." (92% agreed) 5. "factors related to human performance lead to critical information not being perceived." (88% agreed) 6. "Switching between monitors from different manufacturers is difficult." (88% agreed). The ratings of all statements differed significantly from neutral (all p < 0.03).
Conclusion: This study provides an overview of the problems anesthesiologists face in patient monitoring. Some of the issues, to our knowledge, were not previously identified as common problems in patient monitoring, e.g., hardware problems (e.g., cable entanglement and worn connectors), human factor aspects (e.g., fatigue and distractions), and systemic factor aspects (e.g., insufficient standardization between manufacturers). An ideal monitor should transfer the relevant patient monitoring information as efficiently as possible, prevent false positive alarms, and use technologies designed to improve the problems in patient monitoring.
Keywords: Patient monitoring; Patient safety; Qualitative research; Signal processing; Situation awareness.
Conflict of interest statement
The authors DWT, DRS and CBN are in a Joint Development Agreement with Philips Healthcare (Koninklijke Philips N. V, Amsterdam, The Netherlands). Within the framework of this agreement, a product based on the Visual Patient concept shall be developed. If successful, the authors DWT and CBN could receive royalties. All other authors declare that they have no competing interests.
Figures
References
-
- World Alliance for Patient Safety . WHO guidelines for safe surgery. Geneva: Switzerland World Health Organization; 2008.
-
- Endsley MR. Toward a theory of situation awareness in dynamic systems human factors. Hum Factors. 1995;37:32–64. doi: 10.1518/001872095779049543. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
