

Acute Dysnatremias - a dangerous and overlooked clinical problem
- PMID: 31138251
- PMCID: PMC6540386
- DOI: 10.1186/s13049-019-0633-3
Acute Dysnatremias - a dangerous and overlooked clinical problem
Abstract
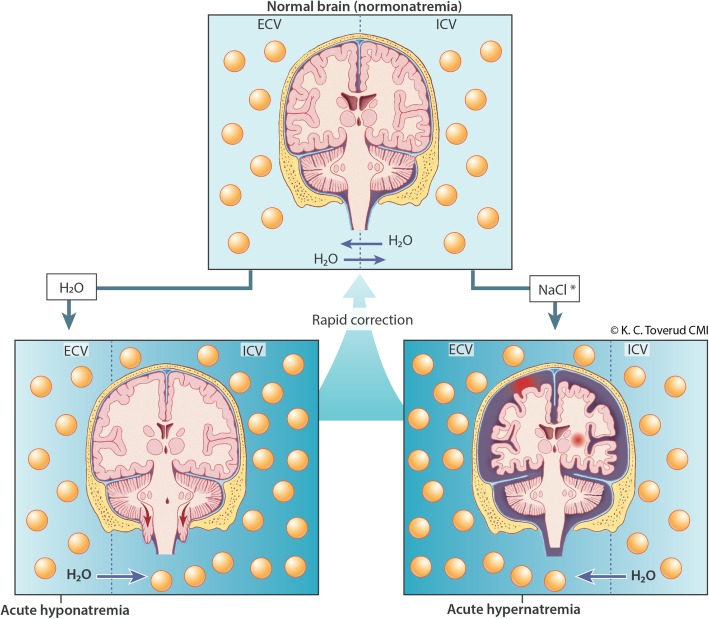
Background: Dysnatremias are common electrolyte disturbances with significant morbidity and mortality. In chronic dysnatremias a slow correction rate (<10 mmol/L/24 h) is indicated to avoid neurological complications. In acute dysnatremias (occurring <48 h) a rapid correction rate may be indicated. Most guidelines do not differ between acute and chronic dysnatremias. In this review, we focus on the evidence-based treatment of acute dysnatremias.
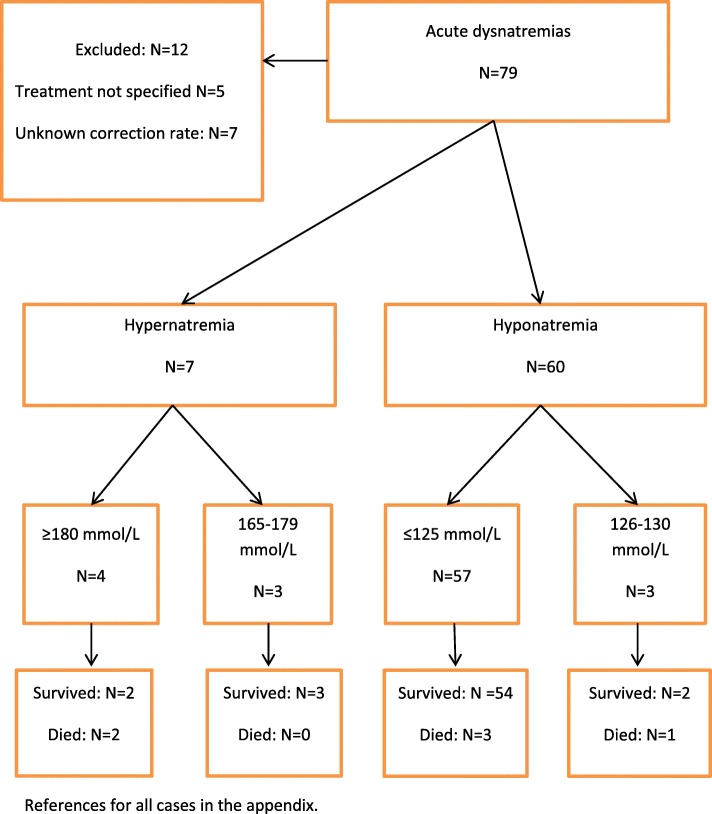
Methods: A literary search in PubMed and Embase. A total of 72 articles containing 79 cases were included, of which 12 cases were excluded due to lack of information.
Results: Of 67 patients (70% women) with acute dysnatremia, 60 had hypo- and 7 had hypernatremia. All patients with hyper- and 88% with hyponatremia had a rapid correction rate (> 10 mmol/L/24 h). The median time of correction was 1 day in patients with hypo- and 2.5 days in patients with hypernatremia. The mortality was 7% in patients with hypo- and 29% in patients with hypernatremia.
Interpretation: Severe acute dysnatremias have significant mortality and require immediate treatment. A rapid correction rate may be lifesaving and is not associated with neurological complications. Chronic dysnatremias, on the other hand, are often compensated and thus less severe. In these cases a rapid correction rate may lead to severe cerebral complications.
Keywords: Acute dysnatremia; Ecstasy-associated hyponatremia; Exercise-associated hyponatremia; Hypernatremia; Hyponatremia; Psychogenic polydipsia; Salt intoxication; Water intoxication.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Preventing neurological complications from dysnatremias in children.Pediatr Nephrol. 2005 Dec;20(12):1687-700. doi: 10.1007/s00467-005-1933-6. Epub 2005 Aug 4. Pediatr Nephrol. 2005. PMID: 16079988 Review.
-
Dysnatremia as a poor prognostic indicator in patients with acute subarachnoid hemorrhage.J Neurosurg Sci. 2017 Aug;61(4):371-379. doi: 10.23736/S0390-5616.16.03411-1. Epub 2015 Oct 23. J Neurosurg Sci. 2017. PMID: 26496416
-
Incidence and prognosis of dysnatremias present on ICU admission.Intensive Care Med. 2010 Feb;36(2):304-11. doi: 10.1007/s00134-009-1692-0. Epub 2009 Oct 22. Intensive Care Med. 2010. PMID: 19847398
-
Clinical Associations of Early Dysnatremias in Critically Ill Neonates and Infants Undergoing Cardiac Surgery.Pediatr Cardiol. 2017 Jan;38(1):149-154. doi: 10.1007/s00246-016-1495-3. Epub 2016 Nov 8. Pediatr Cardiol. 2017. PMID: 27826706
-
Approach and management of dysnatremias in cirrhosis.Hepatol Int. 2018 Nov;12(6):487-499. doi: 10.1007/s12072-018-9894-6. Epub 2018 Sep 10. Hepatol Int. 2018. PMID: 30203382 Review.
Cited by
-
Acute water intoxication in an adult man: 'dental hyponatraemia' revisited.Clin Med (Lond). 2022 Jul;22(4):364-365. doi: 10.7861/clinmed.2022-0141. Clin Med (Lond). 2022. PMID: 35882484 Free PMC article.
-
The Importance of Gender-Related Anticancer Research on Mitochondrial Regulator Sodium Dichloroacetate in Preclinical Studies In Vivo.Cancers (Basel). 2019 Aug 20;11(8):1210. doi: 10.3390/cancers11081210. Cancers (Basel). 2019. PMID: 31434295 Free PMC article. Review.
-
Natraemia variations induced by acute dialysis in critically ill patients: a database study.Sci Rep. 2022 Sep 2;12(1):14930. doi: 10.1038/s41598-022-18897-z. Sci Rep. 2022. PMID: 36056117 Free PMC article.
-
Short-term prognostic models for severe acute kidney injury patients receiving prolonged intermittent renal replacement therapy based on machine learning.BMC Med Inform Decis Mak. 2023 Jul 24;23(1):133. doi: 10.1186/s12911-023-02231-2. BMC Med Inform Decis Mak. 2023. PMID: 37488514 Free PMC article.
-
Outdoor temperature and circulating sodium in children with acute gastroenteritis.Pediatr Res. 2022 Nov;92(5):1270-1273. doi: 10.1038/s41390-022-01947-7. Epub 2022 Feb 17. Pediatr Res. 2022. PMID: 35177815
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
