

Gene-edited stem cells enable CD33-directed immune therapy for myeloid malignancies
- PMID: 31138698
- PMCID: PMC6575599
- DOI: 10.1073/pnas.1819992116
Gene-edited stem cells enable CD33-directed immune therapy for myeloid malignancies
Erratum in
-
Correction for Borot et al., Gene-edited stem cells enable CD33-directed immune therapy for myeloid malignancies.Proc Natl Acad Sci U S A. 2019 Jul 16;116(29):14780-14781. doi: 10.1073/pnas.1909768116. Epub 2019 Jul 8. Proc Natl Acad Sci U S A. 2019. PMID: 31285318 Free PMC article. No abstract available.
Abstract
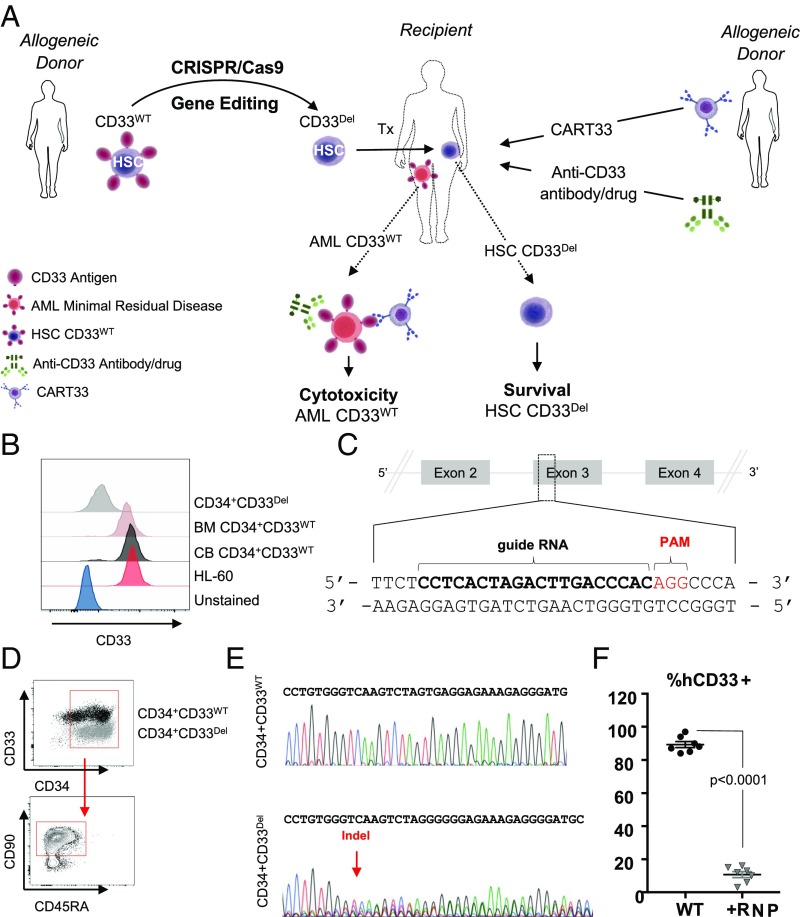
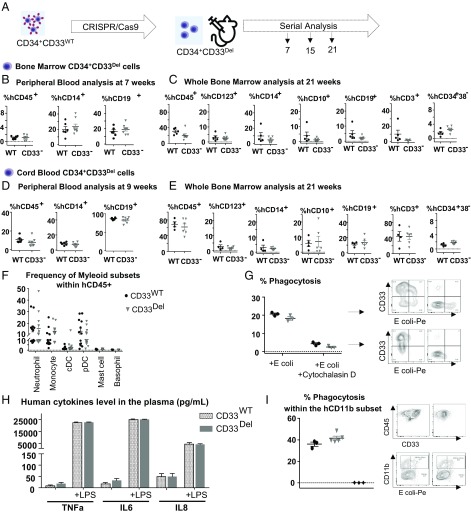
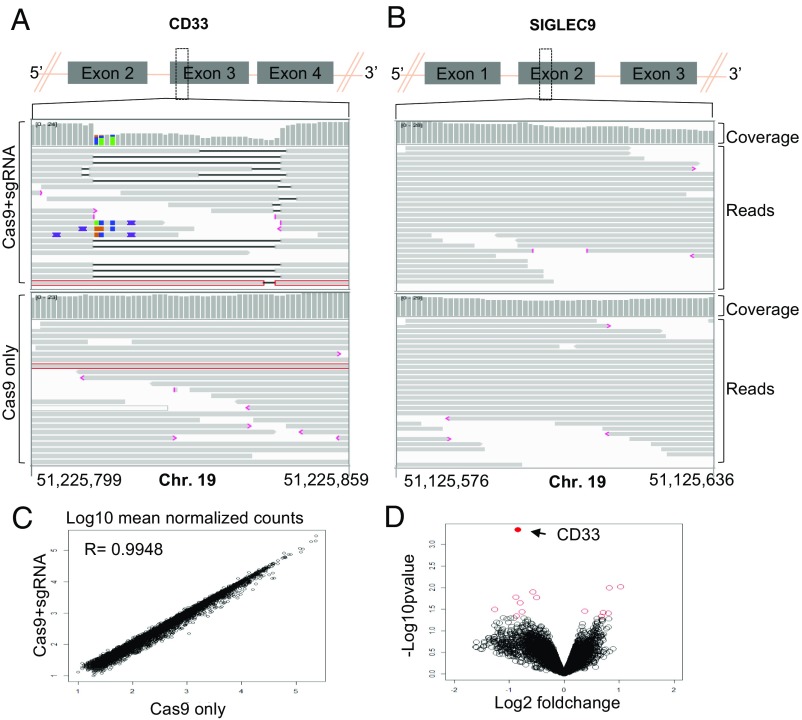
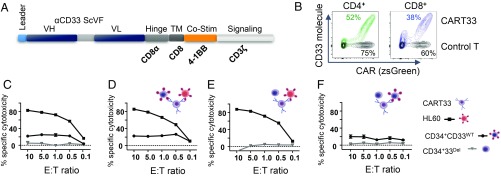
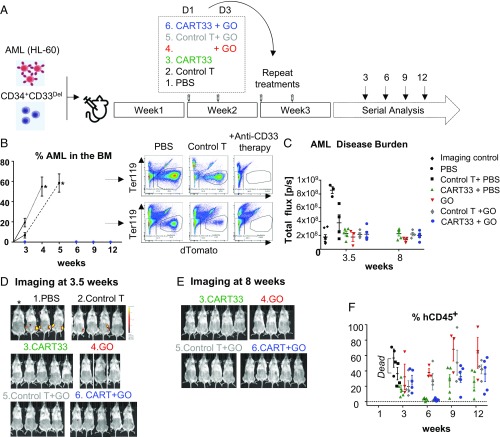
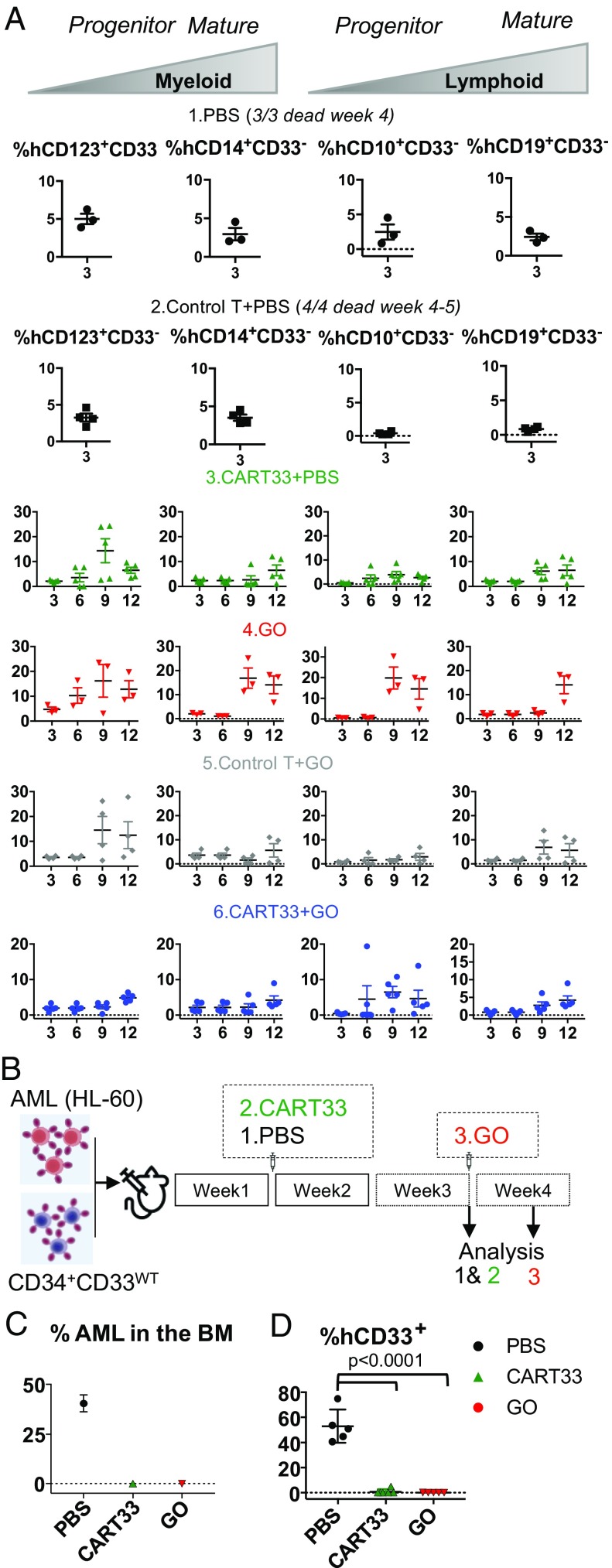
Antigen-directed immunotherapies for acute myeloid leukemia (AML), such as chimeric antigen receptor T cells (CAR-Ts) or antibody-drug conjugates (ADCs), are associated with severe toxicities due to the lack of unique targetable antigens that can distinguish leukemic cells from normal myeloid cells or myeloid progenitors. Here, we present an approach to treat AML by targeting the lineage-specific myeloid antigen CD33. Our approach combines CD33-targeted CAR-T cells, or the ADC Gemtuzumab Ozogamicin with the transplantation of hematopoietic stem cells that have been engineered to ablate CD33 expression using genomic engineering methods. We show highly efficient genetic ablation of CD33 antigen using CRISPR/Cas9 technology in human stem/progenitor cells (HSPC) and provide evidence that the deletion of CD33 in HSPC doesn't impair their ability to engraft and to repopulate a functional multilineage hematopoietic system in vivo. Whole-genome sequencing and RNA sequencing analysis revealed no detectable off-target mutagenesis and no loss of functional p53 pathways. Using a human AML cell line (HL-60), we modeled a postremission marrow with minimal residual disease and showed that the transplantation of CD33-ablated HSPCs with CD33-targeted immunotherapy leads to leukemia clearance, without myelosuppression, as demonstrated by the engraftment and recovery of multilineage descendants of CD33-ablated HSPCs. Our study thus contributes to the advancement of targeted immunotherapy and could be replicated in other malignancies.
Keywords: CD33; CRISPR/Cas9; acute myeloid leukemia; chimeric antigen receptor; transplantation.
Copyright © 2019 the Author(s). Published by PNAS.
Conflict of interest statement
Conflict of interest statement: This study was funded by a grant from Vor Biopharma and PureTech Health, which has launched a company called Vor Biopharma. Columbia University owns equity in Vor Biopharma and has licensed technology that is the subject of this study to Vor Biopharma. F.B., A.M.A., and S.M. are coinventors on issued and pending patent applications licensed to Vor Biopharma. S.M. has equity ownership and is on the Scientific Advisory Board of Vor Biopharma. A.R. received funding from PureTech Health.
Figures
References
-
- O’Donnell M. R., et al. , Acute myeloid leukemia, version 3.2017, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc. Netw. 15, 926–957 (2017). - PubMed
-
- Rai K. R., et al. , Treatment of acute myelocytic leukemia: A study by cancer and leukemia group B. Blood 58, 1203–1212 (1981). - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
Miscellaneous
