

Sepsis-associated disseminated intravascular coagulation and its differential diagnoses
- PMID: 31139417
- PMCID: PMC6528221
- DOI: 10.1186/s40560-019-0387-z
Sepsis-associated disseminated intravascular coagulation and its differential diagnoses
Abstract
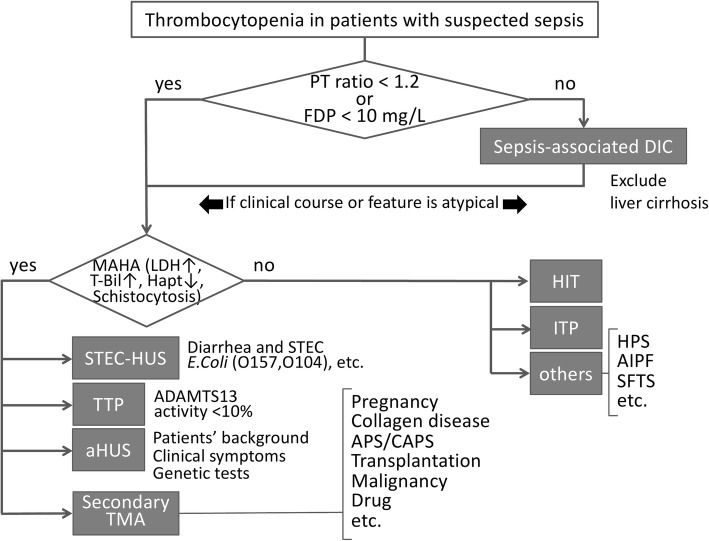
Disseminated intravascular coagulation (DIC) is a common complication in sepsis. Since DIC not only promotes organ dysfunction but also is a strong prognostic factor, its diagnosis at the earliest possible timing is important. Thrombocytopenia is often present in patients with DIC but can also occur in a number of other critical conditions. Of note, many of the rare thrombocytopenic diseases require prompt diagnoses and specific treatments. To differentiate these diseases correctly, the phenotypic expressions must be considered and the different disease pathophysiologies must be understood. There are three major players in the background characteristics of thrombocytopenia: platelets, the coagulation system, and vascular endothelial cells. For example, the activation of coagulation is at the core of the pathogenesis of sepsis-associated DIC, while platelet aggregation is the essential mechanism in thrombotic thrombocytopenic purpura and endothelial damage is the hallmark of hemolytic uremic syndrome. Though each of the three players is important in all thrombocytopenic diseases, one of the three dominant players typically establishes the individual features of each disease. In this review, we introduce the pathogeneses, symptoms, diagnostic measures, and recent therapeutic advances for the major diseases that should be immediately differentiated from DIC in sepsis.
Keywords: Disseminated intravascular coagulation; Hemolytic uremic syndrome; Heparin-induced thrombocytopenia; Sepsis; Thrombotic thrombocytopenic purpura.
Conflict of interest statement
Competing interestsThe authors declare that they have no competing interests.
Figures

References
-
- Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, Bellomo R, Bernard GR, Chiche JD, Coopersmith CM, Hotchkiss RS, Levy MM, Marshall JC, Martin GS, Opal SM, Rubenfeld GD, van der Poll T, Vincent JL, Angus DC. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) JAMA. 2016;23(315):801–810. doi: 10.1001/jama.2016.0287. - DOI - PMC - PubMed
-
- Thiery-Antier N, Binquet C, Vinault S, Meziani F, Boisramé-Helms J, Quenot JP. Is thrombocytopenia an early prognostic marker in septic shock? Crit Care Med. 2016;44:764–772. - PubMed
-
- Claushuis TA, van Vught LA, Scicluna BP, Wiewel MA, Klein Klouwenberg PM, Hoogendijk AJ, Ong DS, Cremer OL, Horn J, Franitza M, Toliat MR, Nürnberg P, Zwinderman AH, Bonten MJ, Schultz MJ, van der Poll T. Thrombocytopenia is associated with a dysregulated host response in critically ill sepsispatients. Blood. 2016;127:3062–3072. doi: 10.1182/blood-2015-11-680744. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
