

Cost-effectiveness of community-based screening and treatment of moderate acute malnutrition in Mali
- PMID: 31139441
- PMCID: PMC6509694
- DOI: 10.1136/bmjgh-2018-001227
Cost-effectiveness of community-based screening and treatment of moderate acute malnutrition in Mali
Abstract
Introduction: Moderate acute malnutrition (MAM) causes substantial child morbidity and mortality, accounting for 4.4% of deaths and 6.0% of disability-adjusted life years (DALY) lost among children under 5 each year. There is growing consensus on the need to provide appropriate treatment of MAM, both to reduce associated morbidity and mortality and to halt its progression to severe acute malnutrition. We estimated health outcomes, costs and cost-effectiveness of four dietary supplements for MAM treatment in children 6-35 months of age in Mali.
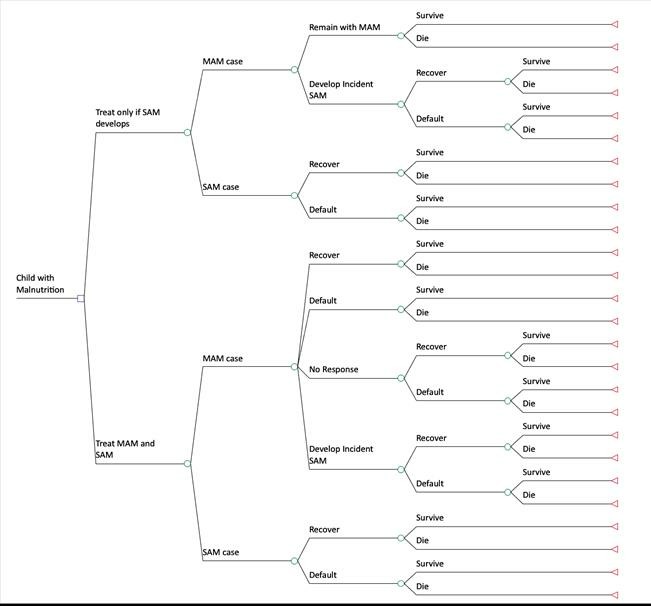
Methods: We conducted a cluster-randomised MAM treatment trial to describe nutritional outcomes of four dietary supplements for the management of MAM: ready-to-use supplementary foods (RUSF; PlumpySup); a specially formulated corn-soy blend (CSB) containing dehulled soybean flour, maize flour, dried skimmed milk, soy oil and a micronutrient pre-mix (CSB++; Super Cereal Plus); Misola, a locally produced, micronutrient-fortified, cereal-legume blend (MI); and locally milled flour (LMF), a mixture of millet, beans, oil and sugar, with a separate micronutrient powder. We used a decision tree model to estimate long-term outcomes and calculated incremental cost-effectiveness ratios (ICERs) comparing the health and economic outcomes of each strategy.
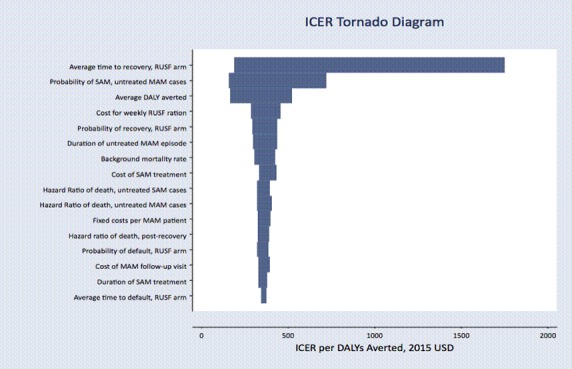
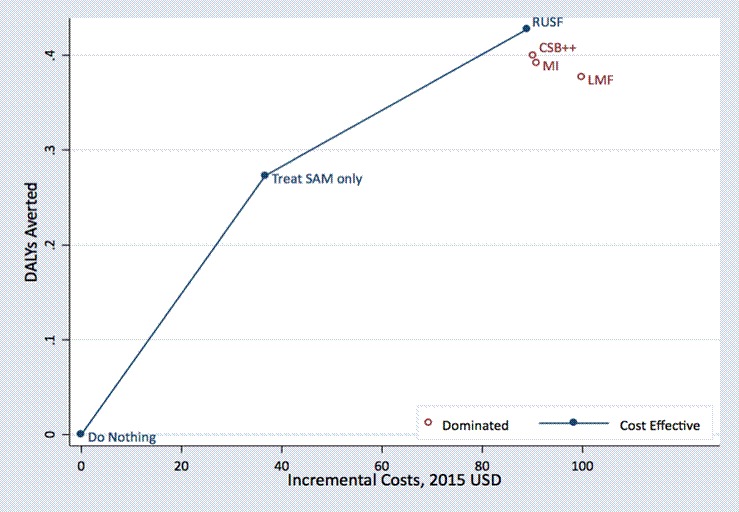
Results: Compared to no MAM treatment, MAM treatment with RUSF, CSB++, MI and LMF reduced the risk of death by 15.4%, 12.7%, 11.9% and 10.3%, respectively. The ICER was US$9821 per death averted (2015 USD) and US$347 per DALY averted for RUSF compared with no MAM treatment.
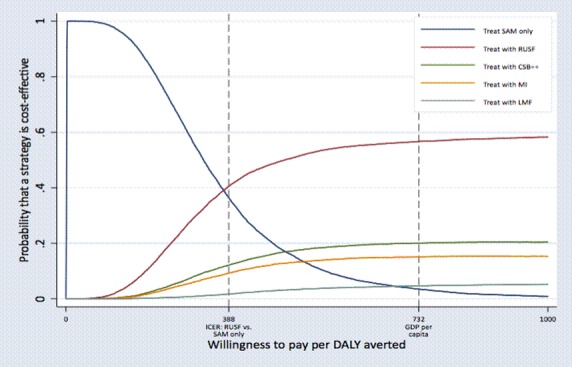
Conclusion: MAM treatment with RUSF is cost-effective across a wide range of willingness-to-pay thresholds.
Trial registration: NCT01015950.
Keywords: CSB++; Mali; PlumpySup; Super Cereal; corn soy blend; cost; cost-effectiveness; moderate acute malnutrition; ready to use supplementary foods.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- UNICEF, World Health Organization, World Bank Joint child malnutrition estimates—2018 edition. New York: UNICEF, WHO and World Bank, 2018.
-
- Navarro-Colorado C, Mason F, Shoham J. Measuring the effectiveness of supplementary feeding programmes in emergencies. London: Humanitarian Practice Network, 2008.