

Risk-adapted moderate hypofractionation of prostate cancer : A prospective analysis of acute toxicity, QOL and outcome in 221 patients
- PMID: 31139841
- PMCID: PMC6763405
- DOI: 10.1007/s00066-019-01477-y
Risk-adapted moderate hypofractionation of prostate cancer : A prospective analysis of acute toxicity, QOL and outcome in 221 patients
Abstract
Purpose: Prostate cancer (PCA) is highly heterogeneous in terms of its oncologic outcome. We therefore aimed to tailor radiation treatment to the risk status by using three different hypofractionated radiation regimen differing in applied dose, use of rectum spacer, inclusion of pelvic lymph nodes (pLN) and use of androgen deprivation therapy (ADT). Here we report on acute toxicity, quality of life (QOL) and oncologic outcome at a median follow-up of 12 months.
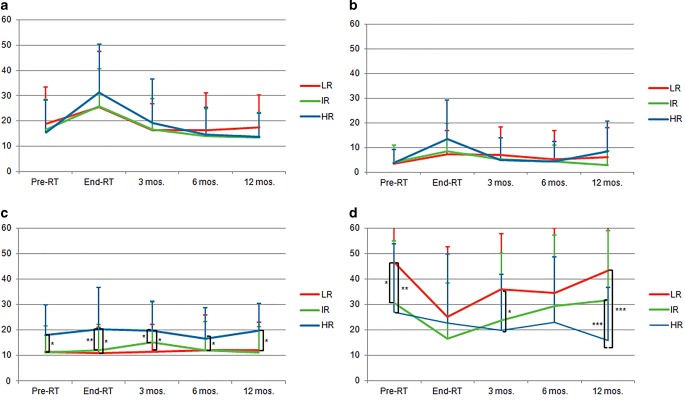
Methods: A total of 221 consecutive PCA patients received hypofractionated intensity-modulated radiotherapy (IMRT). Low-risk (LR) patients were planned to receive 60 Gy in 20 fractions (EQD2α/β1.5 = 77.1 Gy), intermediate-risk (IR) patients 63 Gy in 21 fractions (EQD2α/β1.5 = 81 Gy), and high-risk (HR) patients 67.5 Gy in 25 fractions (EQD2α/β1.5 = 81 Gy) to the prostate and 50 Gy in 25 fractions to the pLN. Acute rectal toxicity was assessed by endoscopy. In addition, toxicity was scored using CTC-AE 4.0 and IPSS score, while QOL was assessed using QLQ-PR25 questionnaires.
Results: Acute CTC reactions were slightly higher in the HR regimen but reverted to baseline at 3 months. GI G2 toxicity was 4%, 0% and 12% for the LR, IR and HR regimen. Compared to IR patients, the increase in toxicity in HR patients was statistically significant (p = 0.002) and mainly caused by a higher incidence of diarrhea presumably due to pelvic EBRT. QOL scores of all domains were worse for the HR regimen (not significant).
Conclusion: Risk-adapted moderate hypofractionation is associated with low GI/GU toxicity. Given the higher rate of pelvic metastases in HR patients, slightly higher transient acute reactions should be outweighed by possible oncological benefits.
Ziel: Das Prostatakarzinom (PCA) ist in Bezug auf das onkologische Ergebnis eine sehr heterogene Erkrankung. Wir etablierten drei risikoadaptierte, hypofraktionierte Bestrahlungsschemata, die sich in der applizierten Dosis, Verwendung von Rektum-Spacern, Einschluss der pelvinen Lymphknoten (pLN) sowie dem Einsatz einer Androgendeprivationstherapie (ADT) unterschieden. Hier berichten wir über die akute Toxizität, Lebensqualität (QOL) sowie das onkologische Ergebnis mit einem medianen Follow-up von 12 Monaten.
Methoden: Eine hypofraktonierte intensitätsmodulierte Radiotherapie (IMRT) erhielten 221 konsekutive PCA-Patienten . Niedrigrisiko(LR)-Patienten erhielten 60 Gy mit 20 Fraktionen (EQD2α/β1,5 = 77,1 Gy), Intermediärrisiko(IR)-Patienten 63 Gy mit 21 Fraktionen (EQD2α/β1,5 = 81 Gy) und Hochrisiko(HR)-Patienten wurden mit 67,5 Gy mit 25 Fraktionen (EQD2α/β1,5 = 81 Gy) auf die Prostata und 50 Gy mit 25 Fraktionen auf die pLN bestrahlt. Die akute rektale Toxizität wurde mittels Endoskopie beurteilt. Weiters wurden CTC-AE V4.0 sowie IPSS-Scores erhoben. Die QOL wurde mittels QLQ-PR25-Fragebögen ermittelt.
Ergebnisse: Die akute Toxizität war in der HR-Gruppe etwas höher, ging allerdings nach 3 Monaten auf das Ursprungsniveau zurück. Die gastrointestinale (GI) G2-Toxizität betrug 4%, 0% und 12% für die LR-, IR- bzw. HR-Gruppe. Verglichen mit den IR-Patienten war der Toxizitätsanstieg der HR-Patienten statistisch signifikant (p = 0,002) und wurde hauptsächlich durch die höhere Diarrhoe-Rate verursacht, vermutlich bedingt durch die pelvine EBRT. Die QOL-Werte aller Domänen waren in der HR-Gruppe etwas schlechter (nicht signifikant).
Schlussfolgerung: Risikoadaptiere moderate Hypofraktionierung ist mit einer niedrigen GI/GU-Toxizität assoziiert. Aufgrund der höheren Rate pelviner Metastasen in HR-Patienten sehen wir die höheren transienten Akutreaktionen durch den möglichen onkologischen Benefit gerechtfertigt.
Keywords: Dose escalation; Hypofractionation; Pelvic lymph nodes; Risk stratification; Spacer.
Conflict of interest statement
A. Schörghofer, M. Groher, J. Karner, A. Kopp, G. Kametriser, T. Kunit, J. Holzinger, F. Sedlmayer and F. Wolf declare that they have no competing interests.
Figures


References
-
- D’Amico AV, Whittington R, Malkowicz SB, Schultz D, Blank K, Broderick GA, Tomaszewski JE, Renshaw AA, Kaplan I, Beard CJ, Wein A. Biochemical outcome after radical prostatectomy, external beam radiation therapy, or interstitial radiation therapy for clinically localized prostate cancer. JAMA. 1998;280(11):969–974. doi: 10.1001/jama.280.11.969. - DOI - PubMed
-
- Hamdy FC, Donovan JL, Lane JA, Mason M, Metcalfe C, Holding P, Davis M, Peters TJ, Turner EL, Martin RM, Oxley J, Robinson M, Staffurth J, Walsh E, Bollina P, Catto J, Doble A, Doherty A, Gillatt D, Kockelbergh R, Kynaston H, Paul A, Powell P, Prescott S, Rosario DJ, Rowe E, Neal DE, ProtecT Study Group 10-year outcomes after monitoring, surgery, or radiotherapy for localized prostate cancer. N Engl J Med. 2016;375(15):1415–1424. doi: 10.1056/NEJMoa1606220. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
