

Safety and efficacy of midazolam nasal spray in the outpatient treatment of patients with seizure clusters-a randomized, double-blind, placebo-controlled trial
- PMID: 31140596
- PMCID: PMC9291143
- DOI: 10.1111/epi.15159
Safety and efficacy of midazolam nasal spray in the outpatient treatment of patients with seizure clusters-a randomized, double-blind, placebo-controlled trial
Abstract
Objective: To evaluate the safety and efficacy of a novel formulation of midazolam administered as a single-dose nasal spray (MDZ-NS) in the outpatient treatment of patients experiencing seizure clusters (SCs).
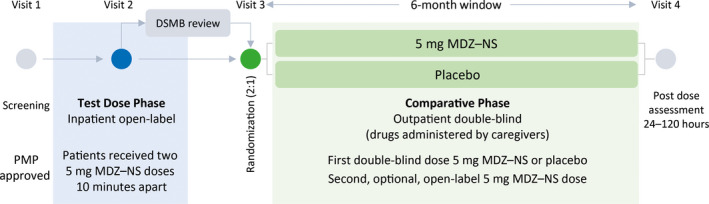
Methods: This was a phase III, randomized, double-blind, placebo-controlled trial (ClinicalTrials.gov NCT01390220) with patients age ≥12 years on a stable regimen of antiepileptic drugs. Following an in-clinic test dose phase (TDP), patients entered an outpatient comparative phase (CP) and were randomized (2:1) to receive double-blind MDZ-NS 5 mg or placebo nasal spray, administered by caregivers when they experienced an SC. The primary efficacy end point was treatment success (seizure termination within 10 minutes and no recurrence 10 minutes to 6 hours after trial drug administration). Secondary efficacy end points were proportion of patients with seizure recurrence 10 minutes to 4 hours, and time-to-next seizure >10 minutes after double-blind drug administration. Safety was monitored throughout.
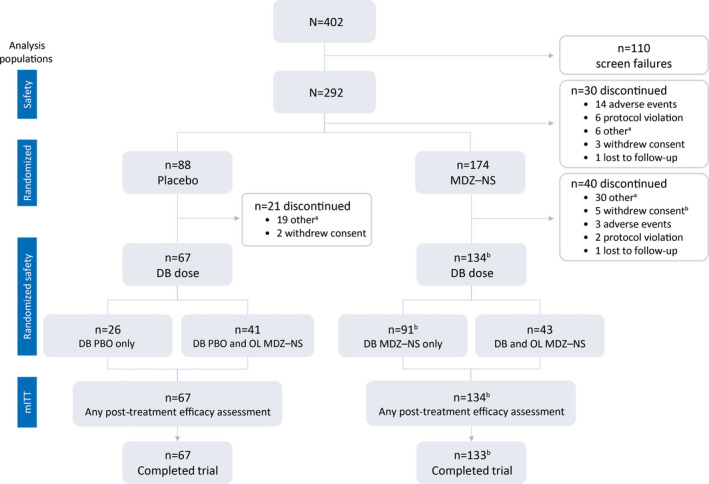
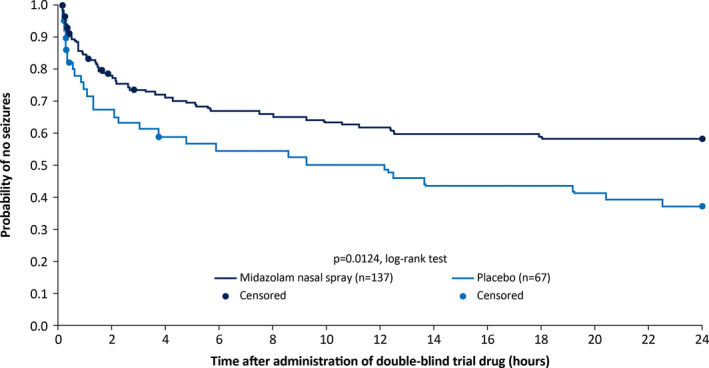
Results: Of 292 patients administered a test dose, 262 patients were randomized, and 201 received double-blind treatment for an SC (n = 134 MDZ-NS, n = 67 placebo, modified intent-to-treat population). A significantly greater proportion of MDZ-NS- than placebo-treated patients achieved treatment success (53.7% vs 34.4%; P = 0.0109). Significantly, fewer MDZ-NS- than placebo-treated patients experienced seizure recurrence (38.1% vs 59.7%; P = 0.0043). Time-to-next seizure analysis showed early separation (within 30 minutes) between MDZ-NS and placebo that was maintained throughout the 24-hour observation period (21% difference at 24 hours; P = 0.0124). Sixteen patients (5.5%) discontinued because of a treatment-emergent adverse event (TEAE) during the TDP and none during the CP. During the CP, 27.6% and 22.4% of patients in the MDZ-NS and placebo groups, respectively, experienced ≥1 TEAE.
Significance: MDZ-NS was superior to placebo in providing rapid, sustained seizure control when administered to patients experiencing an SC in the outpatient setting and was associated with a favorable safety profile.
Keywords: acute intervention; acute repetitive seizures; benzodiazepine; epilepsy; intranasal; rescue.
© 2019 The Authors. Epilepsia published by Wiley Periodicals, Inc. on behalf of International League Against Epilepsy.
Conflict of interest statement
T Meng, WE Pullman, DJ Sequeira, and PJ Van Ess are employees of Proximagen LLC. K Detyniecki has received research support to Yale University for investigator‐initiated studies from Eisai, Sunovion, Acorda, and Upsher‐Smith, and consultation fees from UCB Pharma. JW Wheless has received research grants from Aquestive, Eisai, Greenwich, INSYS Inc, LivaNova, Mallinckrodt, Neuralis, NeuroPace, Shainberg Foundation, and Zogenix; served as a consultant for Aquestive, BioMarin, Eisai, Greenwich, Mallinckrodt, Neuralis, NeuroPace, West, Shire, and Supernus; and participated in speaker's bureau for BioMarin, Eisai, Greenwich, LivaNova, Mallinckrodt, and Supernus. The authors confirm having read the Journal's position on ethical publication and affirm that this report is consistent with their guidelines.
Figures
References
-
- Cereghino JJ. Identification and treatment of acute repetitive seizures in children and adults. Curr Treat Options Neurol. 2007;9:249–55. - PubMed
-
- Sillanpää M, Schmidt D. Seizure clustering during drug treatment affects seizure outcome and mortality of childhood‐onset epilepsy. Brain. 2008;131:938–44. - PubMed
-
- Haut SR. Seizure clusters: characteristics and treatment. Curr Opin Neurol. 2015;28:143–50. - PubMed
-
- Penovich PE, Buelow J, Steinberg K, Sirven J, Wheless J. Burden of seizure clusters on patients with epilepsy and caregivers: survey of patient, caregiver, and clinician perspectives. Neurologist. 2017;22:207–14. - PubMed
-
- Kälviäinen R. Intranasal therapies for acute seizures. Epilepsy Behav. 2015;49:303–6. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
