

Ibrutinib and Venetoclax for First-Line Treatment of CLL
- PMID: 31141631
- PMCID: PMC11827445
- DOI: 10.1056/NEJMoa1900574
Ibrutinib and Venetoclax for First-Line Treatment of CLL
Abstract
Background: Ibrutinib, an inhibitor of Bruton's tyrosine kinase, and venetoclax, an inhibitor of B-cell lymphoma 2 protein, have been approved for patients with chronic lymphocytic leukemia (CLL). Preclinical investigations have indicated potential synergistic interaction of their combination.
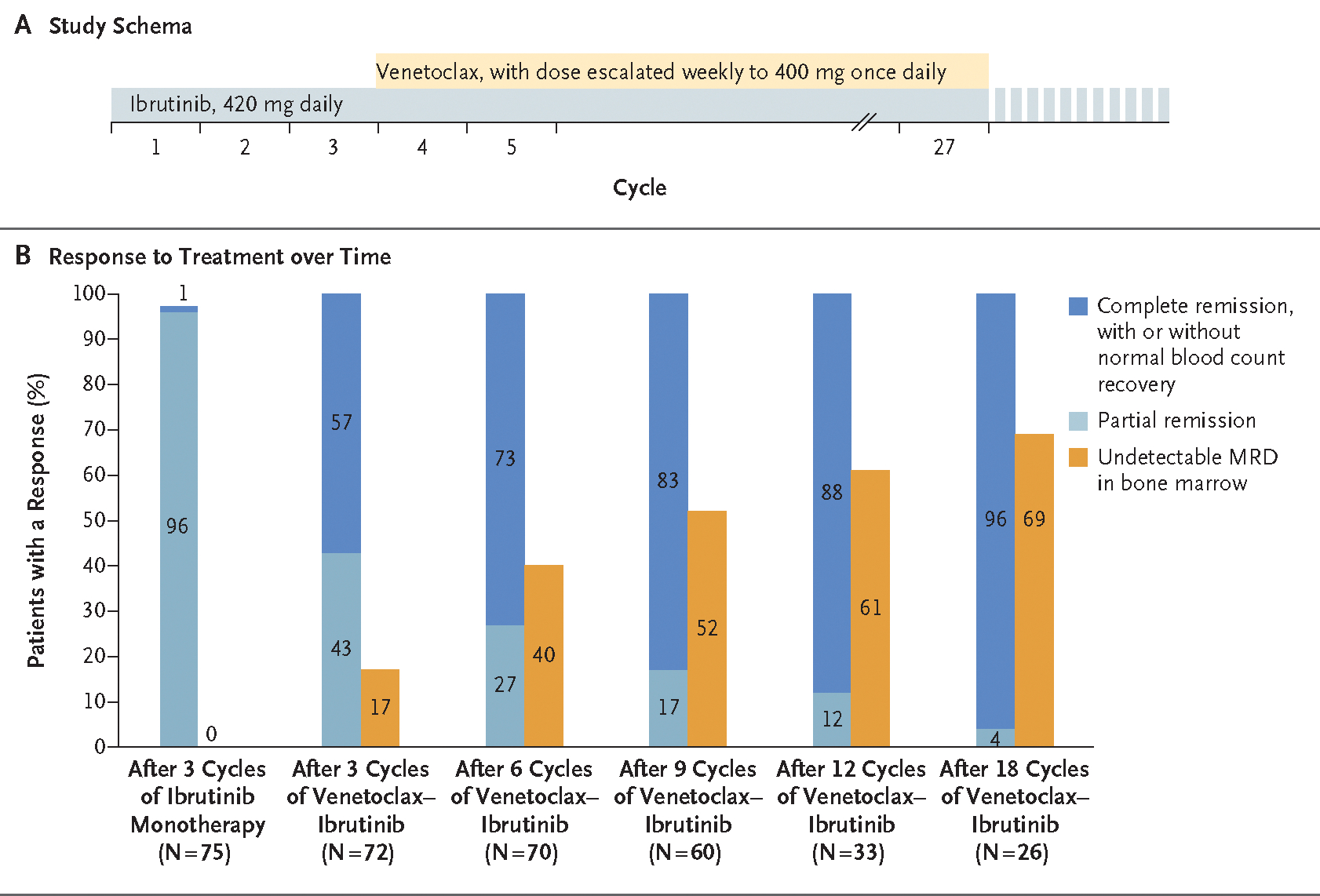
Methods: We conducted an investigator-initiated phase 2 study of combined ibrutinib and venetoclax involving previously untreated high-risk and older patients with CLL. All patients had at least one of the following features: chromosome 17p deletion, mutated TP53, chromosome 11q deletion, unmutated IGHV, or an age of 65 years or older. Patients received ibrutinib monotherapy (420 mg once daily) for 3 cycles, followed by the addition of venetoclax (weekly dose escalation to 400 mg once daily). Combined therapy was administered for 24 cycles. Response assessments were performed according to International Workshop on Chronic Lymphocytic Leukemia 2008 criteria. Minimal residual disease was assessed by means of multicolor flow cytometry in bone marrow (sensitivity, 10-4).
Results: A total of 80 patients were treated. The median age was 65 years (range, 26 to 83). A total of 30% of the patients were 70 years of age or older. Overall, 92% of the patients had unmutated IGHV, TP53 aberration, or chromosome 11q deletion. With combined treatment, the proportions of patients who had complete remission (with or without normal blood count recovery) and remission with undetectable minimal residual disease increased over time. After 12 cycles of combined treatment, 88% of the patients had complete remission or complete remission with incomplete count recovery, and 61% had remission with undetectable minimal residual disease. Responses were noted in older adults and across all high-risk subgroups. Three patients had laboratory evidence of tumor lysis syndrome. The adverse-event profile was similar to what has been reported with ibrutinib and venetoclax.
Conclusions: In this study, combined venetoclax and ibrutinib was an effective oral regimen for high-risk and older patients with CLL. (Funded by AbbVie and others; ClinicalTrials.gov number, NCT02756897.).
Copyright © 2019 Massachusetts Medical Society.
Conflict of interest statement
Disclosure forms provided by the authors are available with the full text of this article at
Figures
Comment in
-
Ibrutinib and Venetoclax - Doubling Down on CLL.N Engl J Med. 2019 May 30;380(22):2169-2171. doi: 10.1056/NEJMe1904362. N Engl J Med. 2019. PMID: 31141640 No abstract available.
-
New first-line options in CLL.Nat Rev Clin Oncol. 2019 Sep;16(9):526-527. doi: 10.1038/s41571-019-0243-z. Nat Rev Clin Oncol. 2019. PMID: 31213701 No abstract available.
-
Ibrutinib and Venetoclax for First-Line Treatment of CLL.N Engl J Med. 2019 Aug 22;381(8):788-789. doi: 10.1056/NEJMc1908754. N Engl J Med. 2019. PMID: 31433936 No abstract available.
References
-
- Hallek M, Shanafelt TD, Eichhorst B. Chronic lymphocytic leukaemia. Lancet 2018;391:1524–37. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous