

Daratumumab plus Lenalidomide and Dexamethasone for Untreated Myeloma
- PMID: 31141632
- PMCID: PMC10045721
- DOI: 10.1056/NEJMoa1817249
Daratumumab plus Lenalidomide and Dexamethasone for Untreated Myeloma
Abstract
Background: Lenalidomide plus dexamethasone is a standard treatment for patients with newly diagnosed multiple myeloma who are ineligible for autologous stem-cell transplantation. We sought to determine whether the addition of daratumumab would significantly reduce the risk of disease progression or death in this population.
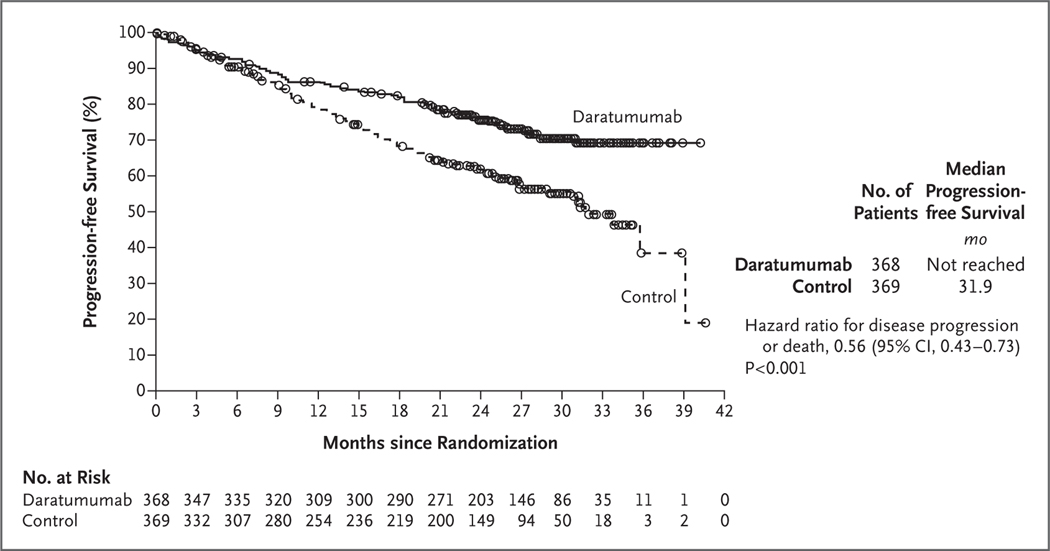
Methods: We randomly assigned 737 patients with newly diagnosed multiple myeloma who were ineligible for autologous stem-cell transplantation to receive daratumumab plus lenalidomide and dexamethasone (daratumumab group) or lenalidomide and dexamethasone alone (control group). Treatment was to continue until the occurrence of disease progression or unacceptable side effects. The primary end point was progression-free survival.
Results: At a median follow-up of 28.0 months, disease progression or death had occurred in 240 patients (97 of 368 patients [26.4%] in the daratumumab group and 143 of 369 patients [38.8%] in the control group). The estimated percentage of patients who were alive without disease progression at 30 months was 70.6% (95% confidence interval [CI], 65.0 to 75.4) in the daratumumab group and 55.6% (95% CI, 49.5 to 61.3) in the control group (hazard ratio for disease progression or death, 0.56; 95% CI, 0.43 to 0.73; P<0.001). The percentage of patients with a complete response or better was 47.6% in the daratumumab group and 24.9% in the control group (P<0.001). A total of 24.2% of the patients in the daratumumab group, as compared with 7.3% of the patients in the control group, had results below the threshold for minimal residual disease (1 tumor cell per 105 white cells) (P<0.001). The most common adverse events of grade 3 or 4 were neutropenia (50.0% in the daratumumab group vs. 35.3% in the control group), anemia (11.8% vs. 19.7%), lymphopenia (15.1% vs. 10.7%), and pneumonia (13.7% vs. 7.9%).
Conclusions: Among patients with newly diagnosed multiple myeloma who were ineligible for autologous stem-cell transplantation, the risk of disease progression or death was significantly lower among those who received daratumumab plus lenalidomide and dexamethasone than among those who received lenalidomide and dexamethasone alone. A higher incidence of neutropenia and pneumonia was observed in the daratumumab group. (Funded by Janssen Research and Development; MAIA ClinicalTrials.gov number, NCT02252172.).
Copyright © 2019 Massachusetts Medical Society.
Figures
Comment in
-
Initial Therapy in Older Patients with Multiple Myeloma.N Engl J Med. 2019 May 30;380(22):2172-2173. doi: 10.1056/NEJMe1904372. N Engl J Med. 2019. PMID: 31141641 No abstract available.
References
-
- Palumbo A, Anderson K. Multiple myeloma. N Engl J Med 2011; 364: 1046–60. - PubMed
-
- Röllig C, Knop S, Bornhäuser M. Multiple myeloma. Lancet 2015; 385:2197–208. - PubMed
-
- Durie BG, Hoering A, Abidi MH, et al. Bortezomib with lenalidomide and dexamethasone versus lenalidomide and dexamethasone alone in patients with newly diagnosed myeloma without intent for immediate autologous stem-cell transplant (SWOG S0777): a randomised, open-label, phase 3 trial. Lancet 2017; 389: 519–27. - PMC - PubMed
-
- Benboubker L, Dimopoulos MA, Dispenzieri A, et al. Lenalidomide and dexamethasone in transplant-ineligible patients with myeloma. N Engl J Med 2014; 371: 906–17. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical