

Hepatitis E Virus Drug Development
- PMID: 31141919
- PMCID: PMC6631701
- DOI: 10.3390/v11060485
Hepatitis E Virus Drug Development
Abstract
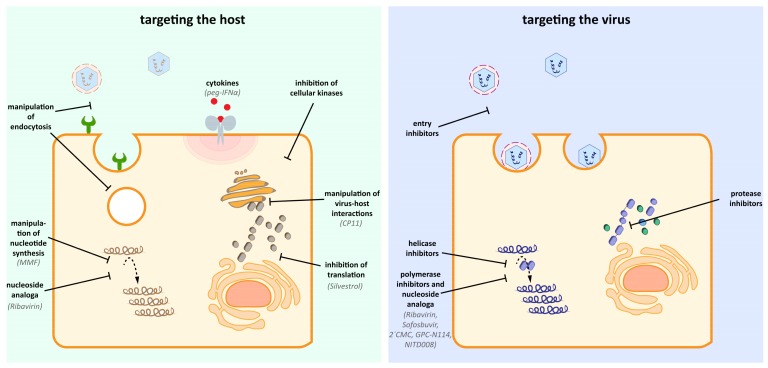
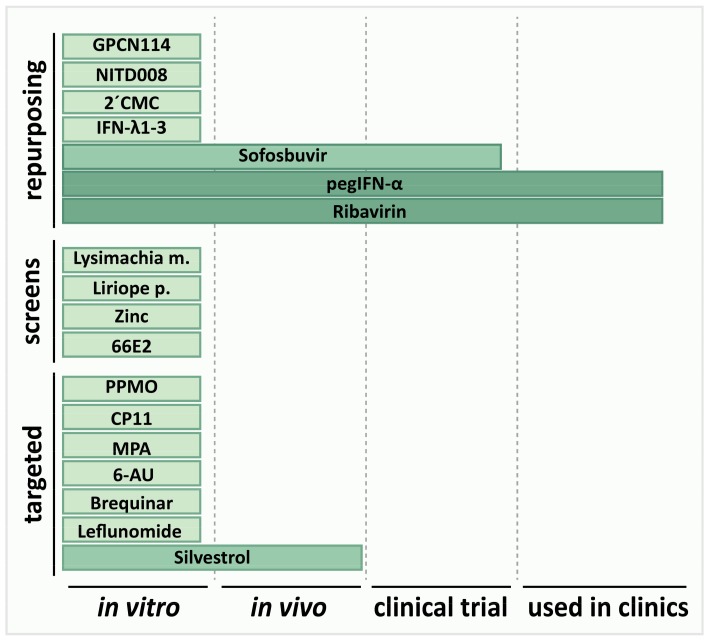
Hepatitis E virus (HEV) is an underestimated disease, leading to estimated 20 million infections and up to 70,000 deaths annually. Infections are mostly asymptomatic but can reach mortality rates up to 25% in pregnant women or become chronic in immunocompromised patients. The current therapy options are limited to the unspecific antivirals Ribavirin (RBV) and pegylated Interferon-α (pegIFN-α). RBV leads to viral clearance in only 80% of patients treated, and is, similar to pegIFN-α, contraindicated in the major risk group of pregnant women, emphasizing the importance of new therapy options. In this review, we focus on the urgent need and current efforts in HEV drug development. We provide an overview of the current status of HEV antiviral research. Furthermore, we discuss strategies for drug development and the limitations of the approaches with respect to HEV.
Keywords: antivirals; drug development; hepatitis E virus; ribavirin; sofosbuvir; therapy; vaccine.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Spina A., Lenglet A., Beversluis D., de Jong M., Vernier L., Spencer C., Andayi F., Kamau C., Vollmer S., Hogema B., et al. A large outbreak of Hepatitis E virus genotype 1 infection in an urban setting in Chad likely linked to household level transmission factors, 2016–2017. PLoS ONE. 2017;12:e0188240. doi: 10.1371/journal.pone.0188240. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
