

Calcitonin negative Medullary Thyroid Carcinoma: a challenging diagnosis or a medical dilemma?
- PMID: 31142313
- PMCID: PMC6541563
- DOI: 10.1186/s12902-019-0367-2
Calcitonin negative Medullary Thyroid Carcinoma: a challenging diagnosis or a medical dilemma?
Abstract
Background: Medullary thyroid carcinoma is a neuroendocrine tumor belonging form a malignant growth of the thyroid parafollicular C-cells, representing from 1 to 10% of all thyroid cancer. The biochemical activity of medullary thyroid carcinoma includes the production of calcitonin and carcinoembryogenic antigen, which are sensitive tumor markers, facilitating the diagnosis, follow-up and prognostication. The diagnosis is reached through the identification of high basal calcitonin serum level or after pentagastrin stimulation test. Medullary thyroid carcinoma is able to produce other relevant biomarkers as procalcitonin, carcinoembryionic antigen and chromogranin A. In Literature are described few cases of medullary thyroid carcinoma without elevation of serum calcitonin, an extremely rare event. The aim of this study was to analyse the presentation, the main features and therapeutic management of medullary thyroid carcinoma associated with negative serum calcitonin levels.
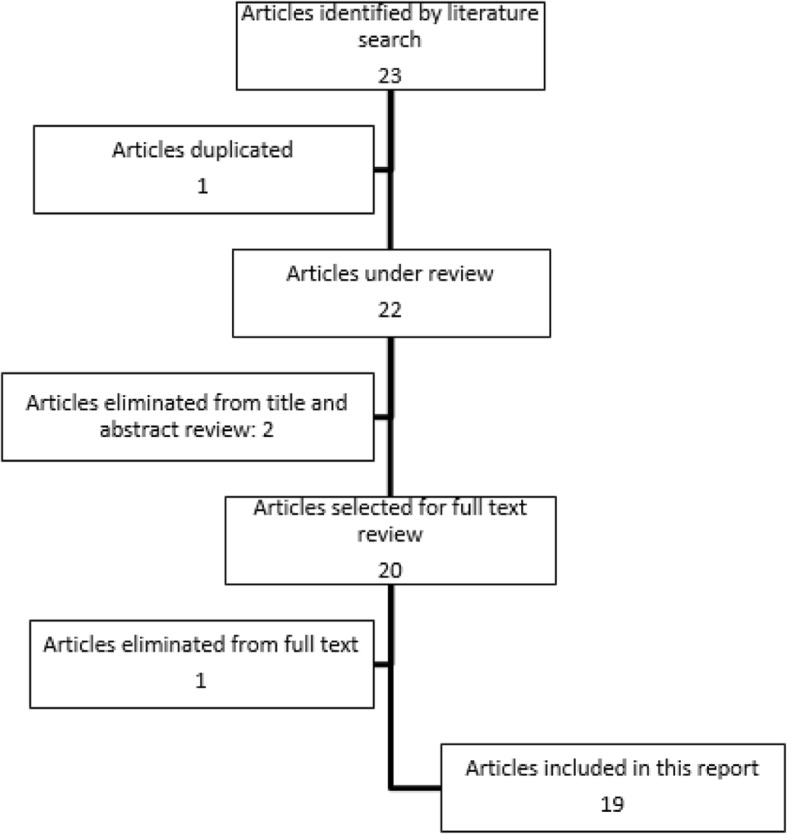
Methods: Using the PubMed database, a systematic review of the current Literature was carried out, up to February 2018. Finally, nineteen articles met our inclusion criteria and were selected according to the modified Newcastle-Ottawa scale.
Results: Fourty-nine patients with definitive pathology confirming medullary thyroid carcinoma and with calcitonin serum level in the normal range were identified (24 female, 24 male and not reported gender in 1 case). Mean age was 51.7 years. Serum calcitonin levels were reported for 20 patients with a mean value of 8.66 pg/mL and a range of 0.8-38 pg/mL. Despite the low or undetectable calcitonin serum level, at immunochemistry in almost the half of the cases reported by the Authors, the tumors presented diffuse or focal positivity for calcitonin and carcinoembryionic antigen, while was reported a chromogranin A positivity in 41 of the 43 tested patients.
Conclusions: Calcitonin negative medullary thyroid carcinoma is an extremely rare pathology. The diagnosis and the surveillance is often challenging and delayed, due to the lack of elevation of serum markers as calcitonin and carcinoembryionic antigen. Further studies are needed, to better define options for management of non secretory medullary thyroid carcinoma and to identify new and reliable biomarkers associated to diagnosis and relapse of this medical dilemma.
Keywords: Calcitonin; Calcitonin negative; Carcinoembryonic antigen; Chromogranin a; Medullary thyroid carcinoma; Procalcitonin; Thyroid nodule.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Medullary thyroid carcinoma with double negative calcitonin and CEA: a case report and update of literature review.BMC Endocr Disord. 2019 Oct 16;19(1):103. doi: 10.1186/s12902-019-0435-7. BMC Endocr Disord. 2019. PMID: 31619220 Free PMC article. Review.
-
Diagnostic value of selected biochemical markers in the detection of recurrence of medullary thyroid cancer - comparison of calcitonin, procalcitonin, chromogranin A, and carcinoembryonic antigen.Endokrynol Pol. 2017;68(4):434-437. doi: 10.5603/EP.a2017.0038. Epub 2017 Jun 6. Endokrynol Pol. 2017. PMID: 28585679
-
Procalcitonin measurement to screen medullary thyroid carcinoma: A prospective evaluation in a series of 2705 patients with thyroid nodules.Eur J Clin Invest. 2018 Jun;48(6):e12934. doi: 10.1111/eci.12934. Epub 2018 Apr 20. Eur J Clin Invest. 2018. PMID: 29635700 Free PMC article.
-
Predictive value of serum calcitonin levels for preoperative diagnosis of medullary thyroid carcinoma in a cohort of 5817 consecutive patients with thyroid nodules.J Clin Endocrinol Metab. 2007 Feb;92(2):450-5. doi: 10.1210/jc.2006-1590. Epub 2006 Nov 21. J Clin Endocrinol Metab. 2007. PMID: 17119000
-
Clinical challenges with calcitonin-negative medullary thyroid carcinoma: three case reports and a review of the literature.Ann R Coll Surg Engl. 2022 Mar;104(3):221-230. doi: 10.1308/rcsann.2020.7118. Epub 2021 Nov 12. Ann R Coll Surg Engl. 2022. PMID: 34767473 Free PMC article. Review.
Cited by
-
Incidental detection of multiple endocrine neoplasia and medullary thyroid carcinoma before starting GLP-1 agonist: A case report.Heliyon. 2024 Jun 22;10(12):e33420. doi: 10.1016/j.heliyon.2024.e33420. eCollection 2024 Jun 30. Heliyon. 2024. PMID: 39015810 Free PMC article.
-
A prediction model for the 5-year, 10-year and 20-year mortality of medullary thyroid carcinoma patients based on lymph node ratio and other predictors.Front Surg. 2023 Jan 13;9:1044971. doi: 10.3389/fsurg.2022.1044971. eCollection 2022. Front Surg. 2023. PMID: 36713658 Free PMC article.
-
Diagnostic dilemma in a patient with history of medullary thyroid carcinoma and abnormal serum liver enzymes; a case report with six years follow up.BMC Endocr Disord. 2023 Aug 30;23(1):186. doi: 10.1186/s12902-023-01439-7. BMC Endocr Disord. 2023. PMID: 37649029 Free PMC article.
-
Liquid Biopsies in Follicular Thyroid Carcinomas-A Brief Report.Diagnostics (Basel). 2024 Jul 22;14(14):1577. doi: 10.3390/diagnostics14141577. Diagnostics (Basel). 2024. PMID: 39061714 Free PMC article.
-
The quality of life after trans oral video-assisted thyroidectomy and cervical thyroidectomy: a systematic review and meta-analysis.Front Surg. 2023 May 17;10:1116473. doi: 10.3389/fsurg.2023.1116473. eCollection 2023. Front Surg. 2023. PMID: 37266003 Free PMC article. Review.
References
-
- Conzo G, Mauriello C, Docimo G, Gambardella C, Thomas G, Cavallo F, Tartaglia E, Napolitano S, Varriale R, Rossetti G, Fei L, Santini L. Clinicopathological pattern of lymph node recurrence of papillary thyroid cancer. Implications for surgery. Int J Surg. 2014;12(Suppl 1):S194–S197. doi: 10.1016/j.ijsu.2014.05.010. - DOI - PubMed
-
- Conzo G, Tartaglia E, Avenia N, Calò PG, de Bellis A, Esposito K, Gambardella C, Iorio S, Pasquali D, Santini L, Sinisi MA, Sinisi AA, Testini M, Polistena A, Bellastella G. Role of prophylactic central compartment lymph node dissection in clinically N0 differentiated thyroid cancer patients: analysis of risk factors and review of modern trends. World J Surg Oncol. 2016;14:149. doi: 10.1186/s12957-016-0879-4. - DOI - PMC - PubMed
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
