

Integrating postpartum contraceptive counseling and IUD insertion services into maternity care in Nepal: results from stepped-wedge randomized controlled trial
- PMID: 31142344
- PMCID: PMC6542050
- DOI: 10.1186/s12978-019-0738-1
Integrating postpartum contraceptive counseling and IUD insertion services into maternity care in Nepal: results from stepped-wedge randomized controlled trial
Abstract
Background: In Nepal, 54% of women have an unmet need for family planning within the 2 years following a birth. Provision of a long-acting and reversible contraceptive method at the time of birth in health facilities could improve access to postpartum family planning for women who want to space or limit their births. This paper examines the impact of an intervention that introduced postpartum contraceptive counseling in antenatal care and immediate postpartum intra-uterine device (PPIUD) insertion services following institutional delivery, with the intent to eventually integrate PPIUD counseling and insertion services as part of routine maternity care in Nepal.
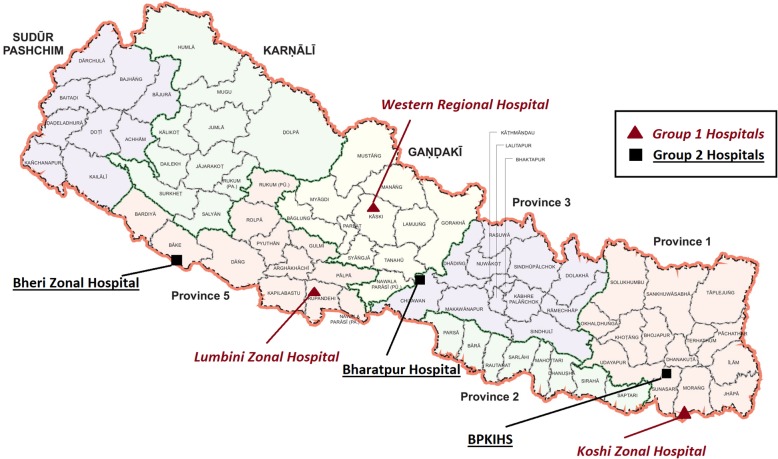
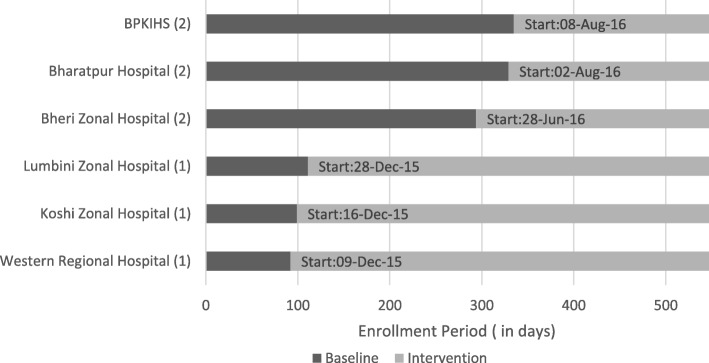
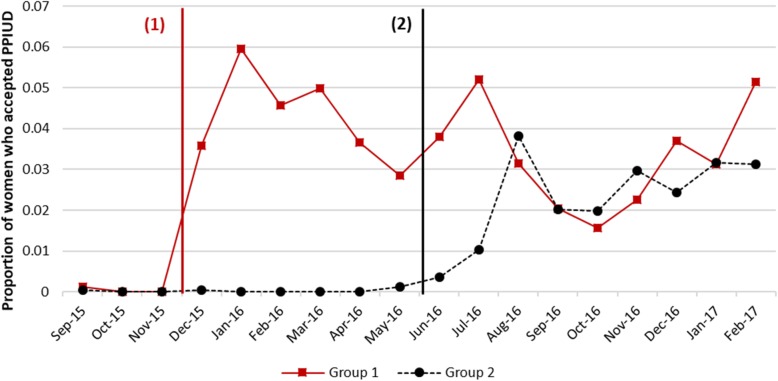
Methods: This study took place in six large tertiary hospitals. All women who gave birth in these hospitals in the 18-month period between September 2015 and March 2017 were asked to participate. A total of 75,587 women (99.6% consent rate) gave consent to be interviewed while in postnatal ward after delivery and before discharge from hospital. We use a stepped-wedge cluster randomized design with randomization of the intervention timing at the hospital level. The baseline data collection began prior to the intervention in all hospitals and the intervention was introduced into the hospitals in two steps, with first group of three hospitals implementing the intervention 3 months after the baseline had begun, and second group of three hospitals implementing the intervention 9 months after the baseline had begun. We estimate the overall effect using a linear regression with a wild bootstrap to estimate valid standard errors given the cluster randomized design. We also estimate the effect of being counseled on PPIUD uptake.
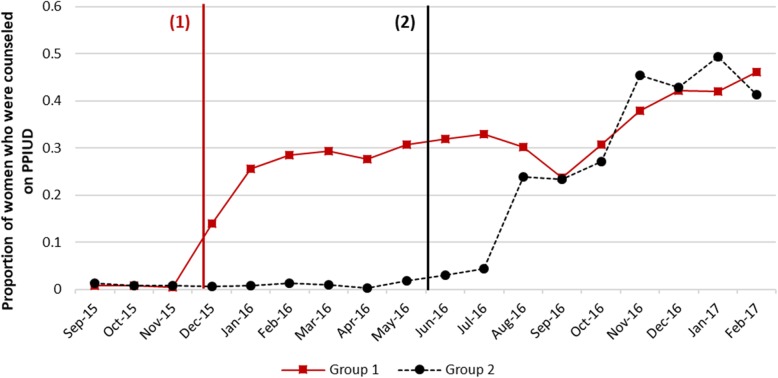
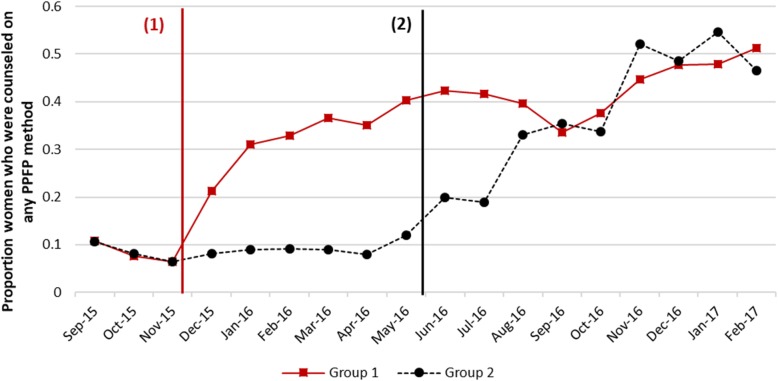
Results: Our Intent-to-Treat analysis shows that being exposed to the intervention increased PPIUD counseling among women by 25 percentage points (pp) [95% CI: 14-40 pp], and PPIUD uptake by four percentage points [95% CI: 3-6 pp]. Our adherence-adjusted estimate shows that, on average, being counseled due to the intervention increased PPIUD uptake by about 17 percentage points [95% CI: 14-40 pp].
Conclusions: The intervention increased PPIUD counseling rates and PPIUD uptake among women in the six study hospitals. If counseling had covered all women in the sample, PPIUD uptake would have been higher. Our results suggest that providing high quality counseling and insertion services generates higher demand for PPIUD services and could reduce unmet need.
Trial registration: Trial registered on March 11, 2016 with ClinicalTrials.gov, NCT02718222 .
Keywords: Counseling; IUD uptake; Impact evaluation; Nepal; Postpartum contraception.
Conflict of interest statement
We have read and understood the
Figures
Similar articles
-
Effect of a postpartum family planning intervention on postpartum intrauterine device counseling and choice: evidence from a cluster-randomized trial in Tanzania.BMC Womens Health. 2020 May 12;20(1):102. doi: 10.1186/s12905-020-00956-0. BMC Womens Health. 2020. PMID: 32398077 Free PMC article. Clinical Trial.
-
The effect of antenatal counseling and intrauterine device insertion services on postpartum contraceptive use in Nepal: Results from a stepped-wedge randomized controlled trial.Contraception. 2020 Jun;101(6):384-392. doi: 10.1016/j.contraception.2019.12.014. Epub 2020 Jan 11. Contraception. 2020. PMID: 31935388 Clinical Trial.
-
Institutionalizing postpartum intrauterine device (IUD) services in Sri Lanka, Tanzania, and Nepal: study protocol for a cluster-randomized stepped-wedge trial.BMC Pregnancy Childbirth. 2016 Nov 21;16(1):362. doi: 10.1186/s12884-016-1160-0. BMC Pregnancy Childbirth. 2016. PMID: 27871269 Free PMC article. Clinical Trial.
-
Expanding access to postpartum contraception.Curr Opin Obstet Gynecol. 2024 Oct 1;36(5):331-337. doi: 10.1097/GCO.0000000000000982. Epub 2024 Aug 2. Curr Opin Obstet Gynecol. 2024. PMID: 39109628 Free PMC article. Review.
-
The effect of family planning counselling on postpartum modern contraceptive uptake in sub-Saharan Africa: a systematic review.Public Health. 2022 May;206:46-56. doi: 10.1016/j.puhe.2022.02.017. Epub 2022 Mar 30. Public Health. 2022. PMID: 35366579
Cited by
-
Effect of Package of Interventions on the Use and Quality of Postpartum Family Planning Services at Yekatit 12 Hospital Medical College (Y12HMC), Addis Ababa, Ethiopia.Health Serv Insights. 2023 Mar 10;16:11786329231160017. doi: 10.1177/11786329231160017. eCollection 2023. Health Serv Insights. 2023. PMID: 36923261 Free PMC article.
-
Individual and facility-level factors associated with women's receipt of immediate postpartum family planning counseling in Ethiopia: results from national surveys of women and health facilities.BMC Pregnancy Childbirth. 2021 Dec 5;21(1):809. doi: 10.1186/s12884-021-04278-3. BMC Pregnancy Childbirth. 2021. PMID: 34865633 Free PMC article.
-
Effect of a postpartum family planning intervention on postpartum intrauterine device counseling and choice: evidence from a cluster-randomized trial in Tanzania.BMC Womens Health. 2020 May 12;20(1):102. doi: 10.1186/s12905-020-00956-0. BMC Womens Health. 2020. PMID: 32398077 Free PMC article. Clinical Trial.
-
'I haven't heard much about other methods': quality of care and person-centredness in a programme to promote the postpartum intrauterine device in Tanzania.BMJ Glob Health. 2021 Jun;6(6):e005775. doi: 10.1136/bmjgh-2021-005775. BMJ Glob Health. 2021. PMID: 34162627 Free PMC article.
-
Clinician and policymaker perspectives on the barriers and enablers to implementing and scaling up integrated postpartum intrauterine contraceptive services within maternity care in Nepal: a qualitative study.Lancet Reg Health Southeast Asia. 2025 May 14;37:100599. doi: 10.1016/j.lansea.2025.100599. eCollection 2025 Jun. Lancet Reg Health Southeast Asia. 2025. PMID: 40487913 Free PMC article.
References
-
- UNFPA. Programme of action of the United Nations international conference on population and development. Cairo: UN; 1994.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
