

Clinically relevant phenotypes in chronic rhinosinusitis
- PMID: 31142355
- PMCID: PMC6542143
- DOI: 10.1186/s40463-019-0350-y
Clinically relevant phenotypes in chronic rhinosinusitis
Erratum in
-
Correction to: Clinically relevant phenotypes in chronic rhinosinusitis.J Otolaryngol Head Neck Surg. 2019 Jul 11;48(1):31. doi: 10.1186/s40463-019-0355-6. J Otolaryngol Head Neck Surg. 2019. PMID: 31296254 Free PMC article.
Abstract
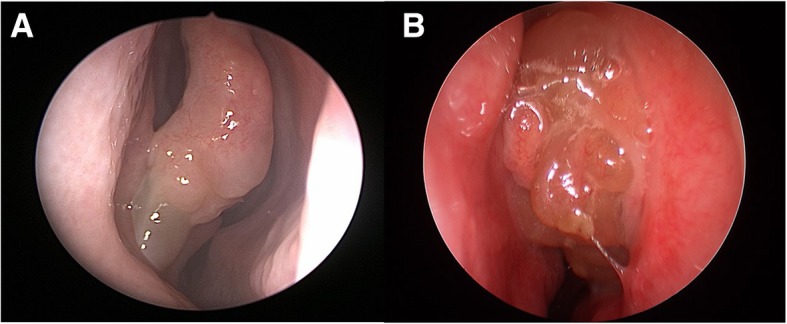
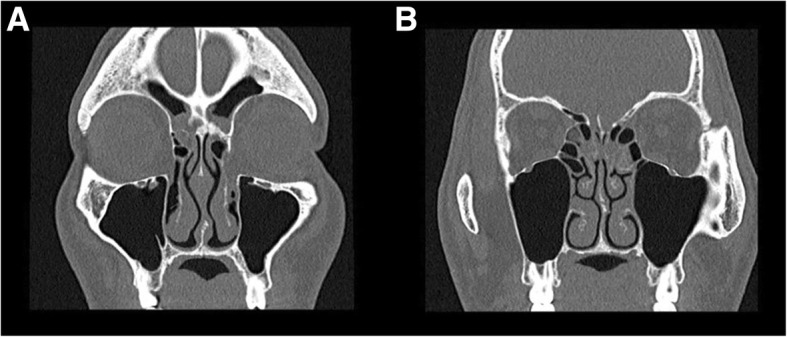
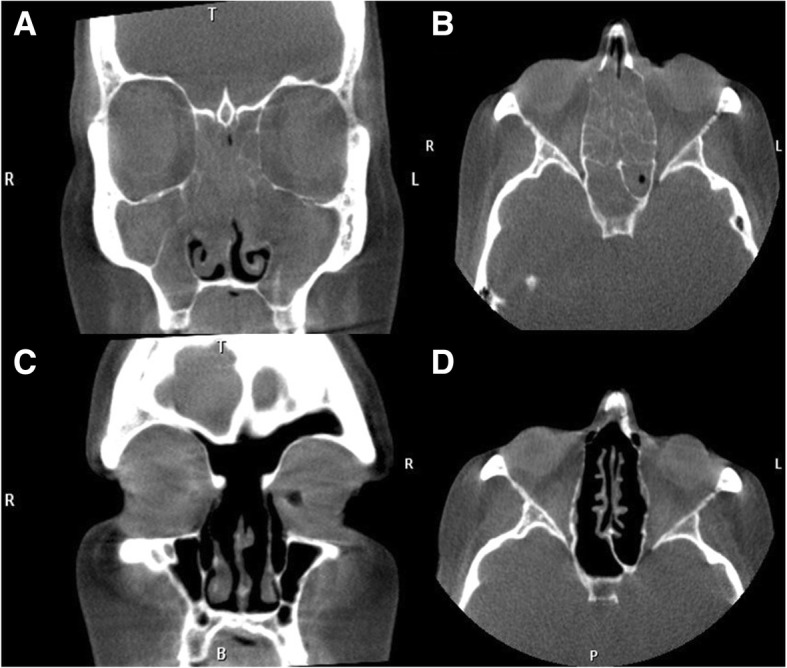
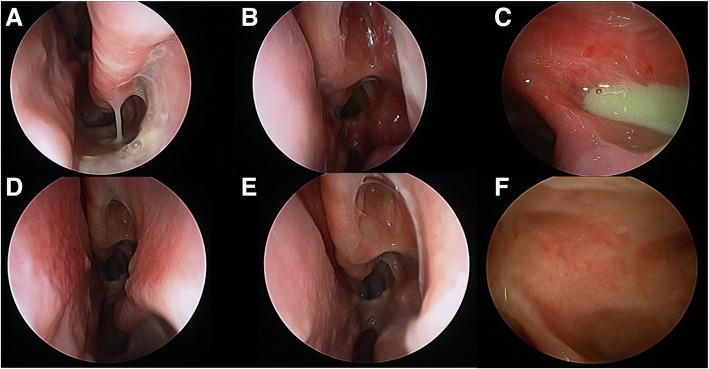
Background: Chronic rhinosinusitis (CRS) is a complex disease that incorporates many different conditions. Currently, primary CRS is considered a disease of broad airway inflammation, however, the previous classification of CRS with and without nasal polyposis fails to adequately classify patients based upon their etiology of illness. Our aim with this review is discuss the clinical presentation, radiology, endoscopy, histopathology, and treatment algorithm of three different phenotypes of primary CRS: central compartment atopic disease, eosinophilic CRS, and non-eosinophilic CRS.
Methods: A narrative review of a tertiary rhinology center's research themes and how they are applied to clinical protocols and practice was assessed.
Discussion: Diagnosis and treatment of upper and lower airway conditions become increasingly important as phenotypes and endotypes are being described. There are well-described therapies to treat the different phenotypes of CRS, based upon the presumed underlying cause of the inflammatory process. Research continues to shed more light on different endotypes and phenotypes of airway inflammation, however, clinical differentiation of CRS can be applied in clinic practice with three simple phenotypes of CRS. Understanding these different phenotypes and their etiologies allows for further management beyond the 'maximum medical therapy and then surgery' approach that has often been used in the management of CRS.
Conflict of interest statement
RH is a consultant with Medtronic, Olympus and NeilMed pharmaceuticals. He has received research grant funding from Meda Pharmaceuticals and Stallergenes. He has been on the speakers’ bureau for BHR, Seqiris, Astra Zeneca, and Glaxo-Smith-Kline and Arthrocare. The remaining authors have no disclosures.
Figures


References
-
- Fokkens W. Lund V, Mullol J. European position paper on R, nasal polyps g. European position paper on rhinosinusitis and nasal polyps 2007. Rhinol Suppl. 2007;20:1–136. - PubMed
-
- Fokkens WJ, Lund VJ, Mullol J, et al. European position paper on rhinosinusitis and nasal polyps 2012. Rhinol Suppl. 2012;23 3 p preceding table of contents, 1-298. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
