

Comparison of diffusion kurtosis imaging versus diffusion weighted imaging in predicting the recurrence of early stage single nodules of hepatocellular carcinoma treated by radiofrequency ablation
- PMID: 31142356
- PMCID: PMC6542145
- DOI: 10.1186/s40644-019-0213-9
Comparison of diffusion kurtosis imaging versus diffusion weighted imaging in predicting the recurrence of early stage single nodules of hepatocellular carcinoma treated by radiofrequency ablation
Abstract
Objective: This study aimed to compare the diffusion kurtosis imaging (DKI) versus diffusion weighted imaging (DWI) in predicting the recurrence of early stage single nodules of hepatocellular carcinoma (HCC) treated by radiofrequency ablation (RFA).
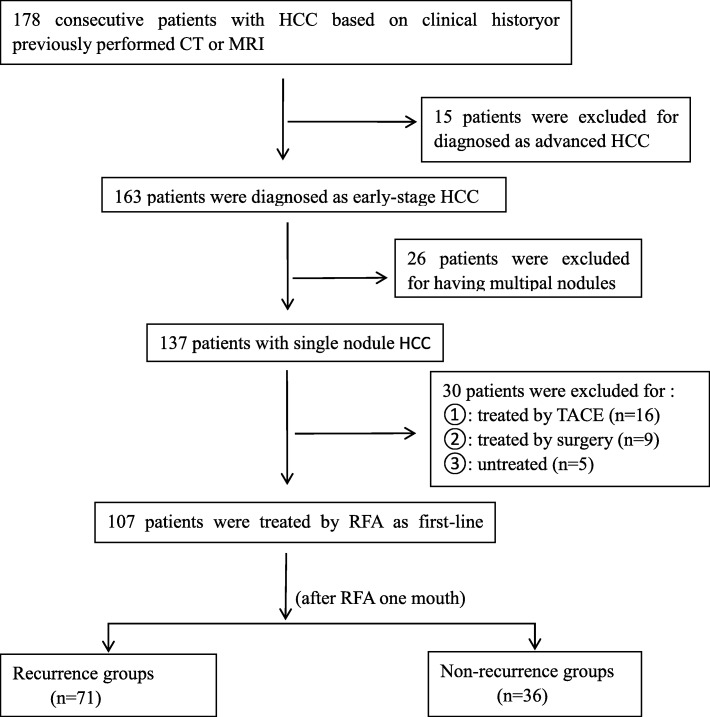
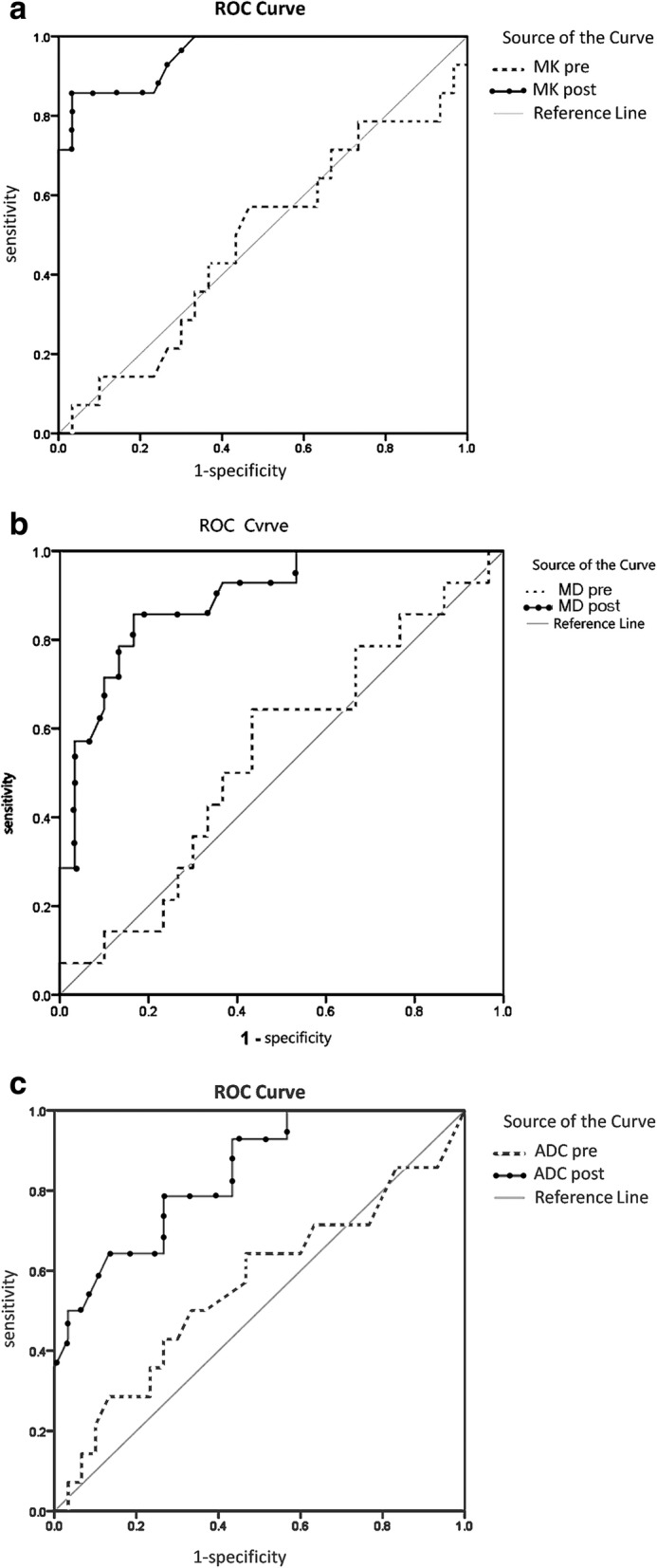
Materials and methods: A retrospective analysis of 107 patients with early stage single nodules of HCC was performed, all patients treated by RFA. Recurrence rate of HCC was recorded after a median follow-up of 36 months. During follow-up, the data of magnetic resonance imaging (MRI), DWI and DKI were obtained in multiple time points. The predictive values of DWI and DKI were analyzed using ROC curves.
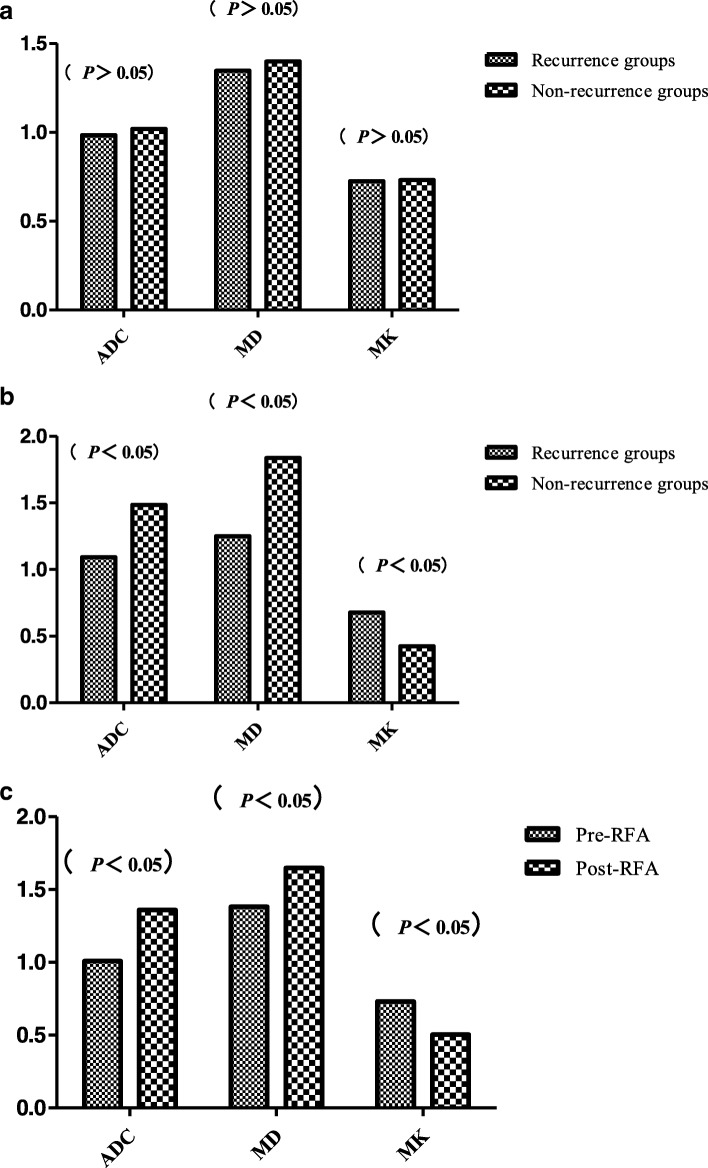
Results: The overall recurrence rate was 66.3% (71/107). The sensitivity, specificity, and AUC for ADC, MD and MK after RFA (78.6, 73.3% and 0.842; 85.7, 83.3% and 0.839; 85.7, 96.7% and 0.956) were higher than before RFA (44.3, 53.3% and 0.560; 51.2, 56.7% and 0.543; 43.6, 67.3% and 0.489). The sensitivity, specificity, and AUC for MK after RFA were 85.7, 96.7%, and 0.956, respectively, which were significantly greater than those of ADC (78.6, 73.3% and 0.842; P < 0.05) and MD (85.7, 83.3% and 0.839).
Conclusions: The prediction efficacy of DKI for the recurrence of early stage single nodules of HCC was better than that of DWI. And, MK was the most sensitive predictor among the DKI.
Keywords: Diffusion kurtosis imaging; Diffusion weighted imaging; Hepatocellular carcinoma; Radiofrequency ablation.
Conflict of interest statement
The authors declare that there are no competing interests.
Figures
Similar articles
-
Diffusion Kurtosis MR Imaging versus Conventional Diffusion-Weighted Imaging for Distinguishing Hepatocellular Carcinoma from Benign Hepatic Nodules.Contrast Media Mol Imaging. 2019 Jul 17;2019:2030147. doi: 10.1155/2019/2030147. eCollection 2019. Contrast Media Mol Imaging. 2019. PMID: 31396023 Free PMC article.
-
Diffusion kurtosis imaging to assess response to treatment in hypervascular hepatocellular carcinoma.AJR Am J Roentgenol. 2015 May;204(5):W543-9. doi: 10.2214/AJR.14.13235. AJR Am J Roentgenol. 2015. PMID: 25905960
-
Comparison of diffusion-weighted imaging mono-exponential mode with diffusion kurtosis imaging for predicting pathological grades of clear cell renal cell carcinoma.Eur J Radiol. 2020 Sep;130:109195. doi: 10.1016/j.ejrad.2020.109195. Epub 2020 Jul 26. Eur J Radiol. 2020. PMID: 32763475
-
Beyond the vascular profile: conventional DWI, IVIM and kurtosis in the assessment of hepatocellular carcinoma.Eur Rev Med Pharmacol Sci. 2020 Jul;24(13):7284-7293. doi: 10.26355/eurrev_202007_21883. Eur Rev Med Pharmacol Sci. 2020. PMID: 32706066 Review.
-
Diffusion Kurtosis Imaging for Assessing the Therapeutic Response of Transcatheter Arterial Chemoembolization in Hepatocellular Carcinoma.J Cancer. 2020 Feb 10;11(8):2339-2347. doi: 10.7150/jca.32491. eCollection 2020. J Cancer. 2020. PMID: 32127960 Free PMC article. Review.
Cited by
-
Value of intravoxel incoherent motion and diffusion kurtosis imaging to differentiate hepatocellular carcinoma and intrahepatic cholangiocarcinoma.World J Gastrointest Oncol. 2025 Aug 15;17(8):108679. doi: 10.4251/wjgo.v17.i8.108679. World J Gastrointest Oncol. 2025. PMID: 40837759 Free PMC article.
-
The Role of Non-Gaussian Models of Diffusion Weighted MRI in Hepatocellular Carcinoma: A Systematic Review.J Clin Med. 2021 Jun 15;10(12):2641. doi: 10.3390/jcm10122641. J Clin Med. 2021. PMID: 34203995 Free PMC article. Review.
-
Predicting the effects of radiotherapy based on diffusion kurtosis imaging in a xenograft mouse model of esophageal carcinoma.Exp Ther Med. 2021 Apr;21(4):327. doi: 10.3892/etm.2021.9758. Epub 2021 Feb 5. Exp Ther Med. 2021. PMID: 33732300 Free PMC article.
-
Application of diffusion kurtosis imaging in differential diagnosis of focal liver lesions.Pol J Radiol. 2023 Oct 4;88:e455-e460. doi: 10.5114/pjr.2023.131911. eCollection 2023. Pol J Radiol. 2023. PMID: 38020499 Free PMC article.
-
Magnetic resonance imaging for treatment response evaluation and prognostication of hepatocellular carcinoma after thermal ablation.Insights Imaging. 2023 May 16;14(1):87. doi: 10.1186/s13244-023-01440-7. Insights Imaging. 2023. PMID: 37188987 Free PMC article. Review.
References
Publication types
MeSH terms
Grants and funding
- 81641074,81171303,30470518,8177182/National Natural Science Foundation of China
- ZR2009CL046,ZR2010HQ029,ZR2016HL40,ZR2017MH037/Natural Science Foundation of Shandong Province
- BS2012YY038/Scientific research award fund for outstanding young and middle-aged scientists in shandong province
- J18KA288/Scientific research program of colleges and universities in shandong province
- 2011WSB29009,2011HW067,2017WS408,2017WS579/Shandong province medical and health science and technology development plan
- 2017YX054/Weifang science and technology development project
- 2012 YD18064/Shandong province science and technology development projection
- 2011HW067/Project of Medicine and Health Development Plan of Shandong Province
- ZR2013HM071/Shandong Provincial Natural Science Foundation of China
- GG201710080117/Key research and development program of shandong province
LinkOut - more resources
Full Text Sources
Medical
