

IL15 by Continuous Intravenous Infusion to Adult Patients with Solid Tumors in a Phase I Trial Induced Dramatic NK-Cell Subset Expansion
- PMID: 31142503
- PMCID: PMC6697593
- DOI: 10.1158/1078-0432.CCR-18-3468
IL15 by Continuous Intravenous Infusion to Adult Patients with Solid Tumors in a Phase I Trial Induced Dramatic NK-Cell Subset Expansion
Abstract
Purpose: The first-in-human clinical trial with human bolus intravenous infusion IL15 (rhIL15) was limited by treatment-associated toxicity. Here, we report toxicity, immunomodulation, and clinical activity of rhIL15 administered as a 10-day continuous intravenous infusion (CIV) to patients with cancers in a phase I trial.
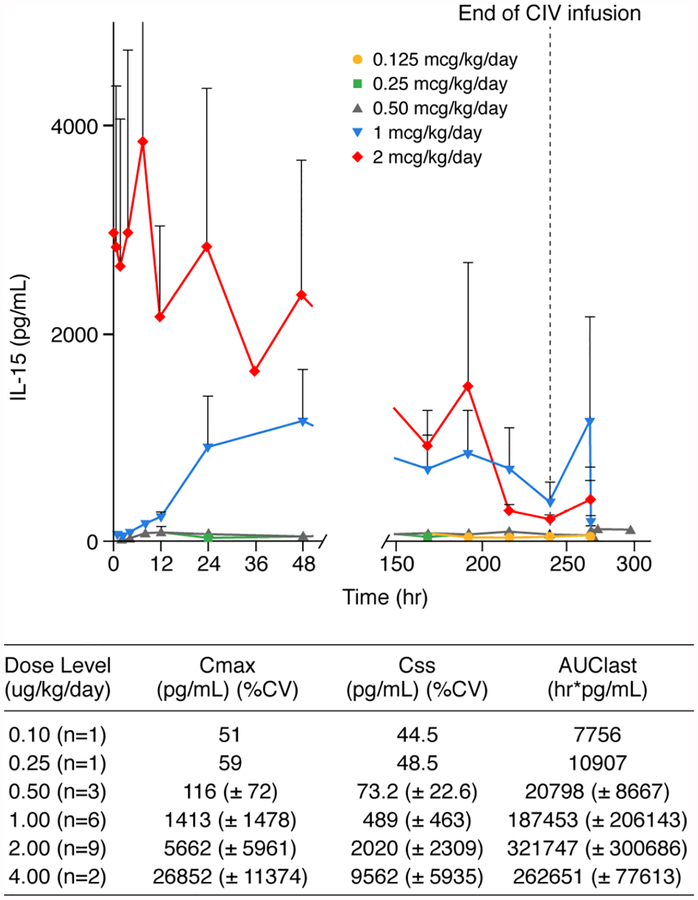
Patients and methods: Patients received treatment for 10 days with CIV rhIL15 in doses of 0.125, 0.25, 0.5, 1, 2, or 4 μg/kg/day. Correlative laboratory tests included IL15 pharmacokinetic (PK) analyses, and assessment of changes in lymphocyte subset numbers.
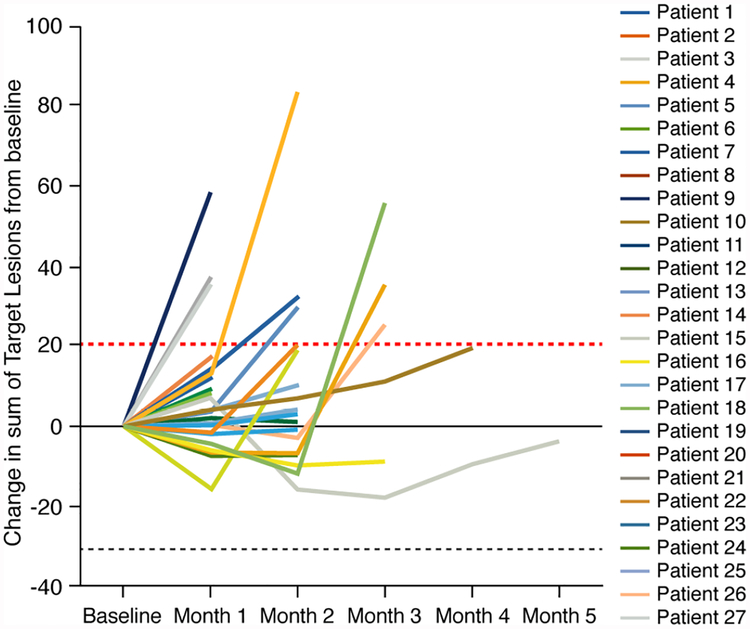
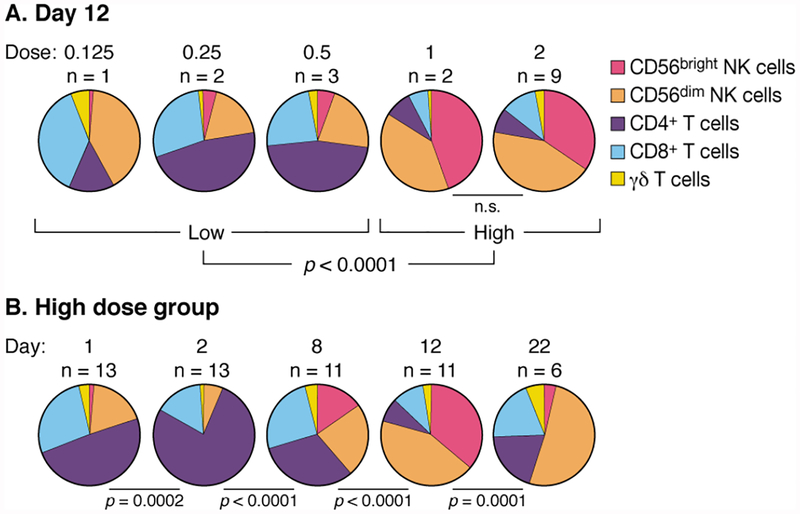
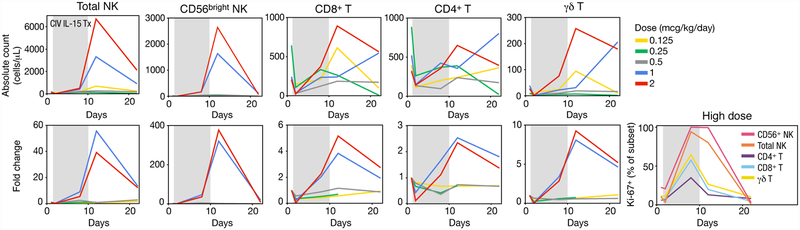
Results: Twenty-seven patients were treated with rhIL15; 2 μg/kg/day was identified as the MTD. There were eight serious adverse events including two bleeding events, papilledema, uveitis, pneumonitis, duodenal erosions, and two deaths (one due to likely drug-related gastrointestinal ischemia). Evidence of antitumor effects was observed in several patients, but stable disease was the best response noted. Patients in the 2 μg/kg/day group had a 5.8-fold increase in number of circulating CD8+ T cells, 38-fold increase in total NK cells, and 358-fold increase in CD56bright NK cells. Serum IL15 concentrations were markedly lower during the last 3 days of infusion.
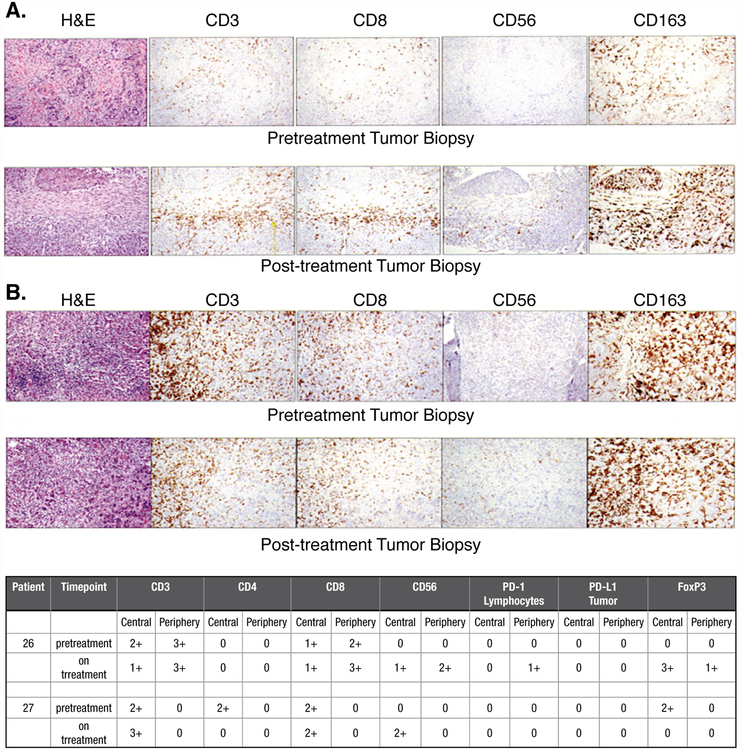
Conclusions: This phase I trial identified the MTD for CIV rhIL15 and defined a treatment regimen that produced significant expansions of CD8+ T and NK effector cells in circulation and tumor deposits. This regimen has identified several biological features, including dramatic increases in numbers of NK cells, supporting trials of IL15 with anticancer mAbs to increase antibody-dependent cell-mediated cytotoxicity and anticancer efficacy.
Trial registration: ClinicalTrials.gov NCT01572493.
©2019 American Association for Cancer Research.
Conflict of interest statement
Figures
References
-
- Choudhury M, Efros M, Mittelman A. Interferons and interleukins in metastatic renal cell carcinoma. Urology 1993; 41:67–72. - PubMed
-
- Kaufman HL, Kirkwood JM, Hodi FS, Agarwala S, Amatruda T, Bines SD, et al. The Society for Immunotherapy of Cancer consensus statement on tumour immunotherapy for the treatment of cutaneous melanoma. Nat Rev Clin Oncol 2013; 10:588–598. - PubMed
-
- Linehan WM, Walther MM, Alexander RB, Rosenberg SA. Adoptive immunotherapy of renal cell carcinoma: studies from the Surgery Branch, National Cancer Institute. Semin Urol 1993; 11:41–43. - PubMed
-
- Atkins MB, Lotze MT, Dutcher JP, Fisher RI, Weiss G, Margolin K, et al. High-dose recombinant interleukin 2 therapy for patients with metastatic melanoma: analysis of 270 patients treated between 1985 and 1993. J Clin Oncol 1999; 17:2105–2116. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
