

Pure Endoscopic Lateral Orbitotomy Approach to the Cavernous Sinus, Posterior, and Infratemporal Fossae: Anatomic Study
- PMID: 31143574
- PMCID: PMC6534734
- DOI: 10.1055/s-0038-1669937
Pure Endoscopic Lateral Orbitotomy Approach to the Cavernous Sinus, Posterior, and Infratemporal Fossae: Anatomic Study
Abstract
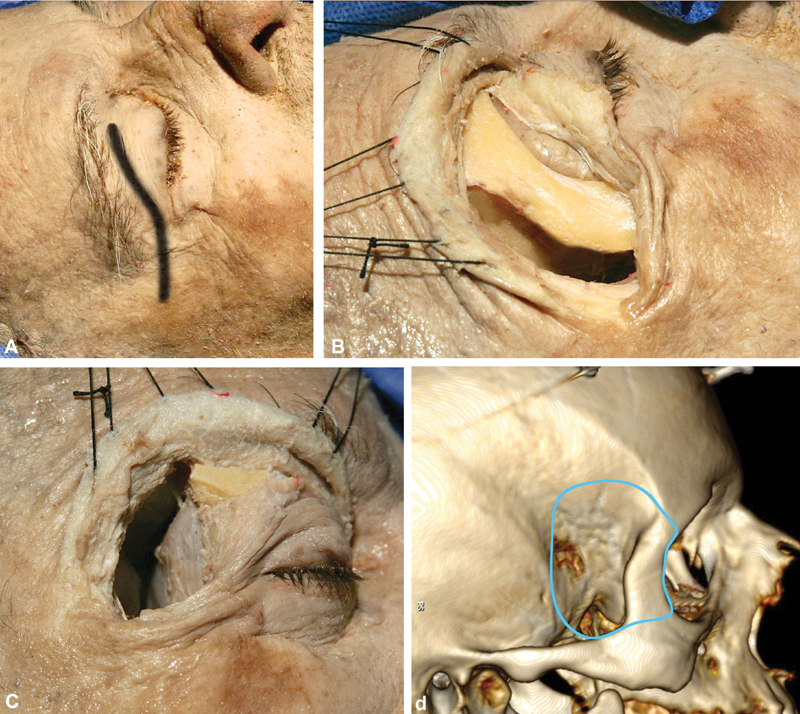
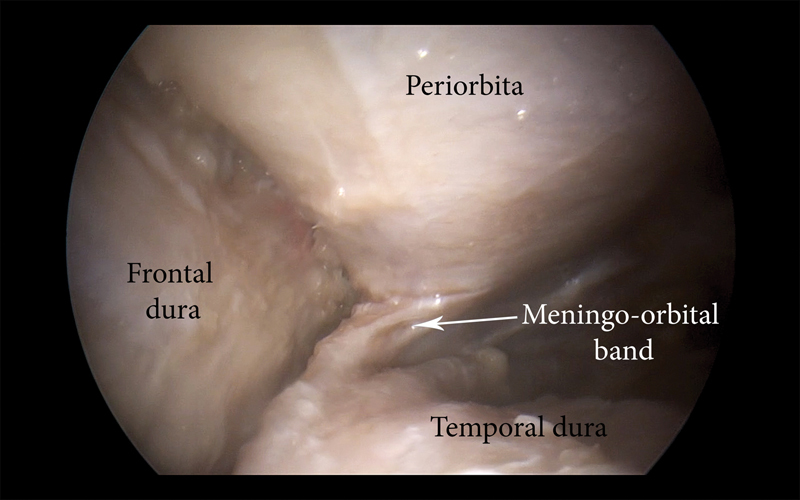
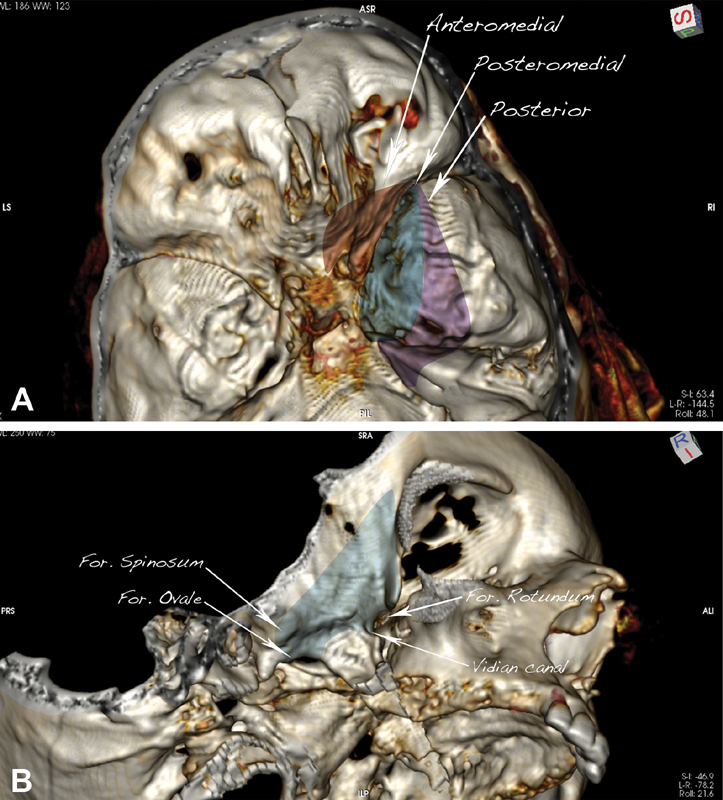
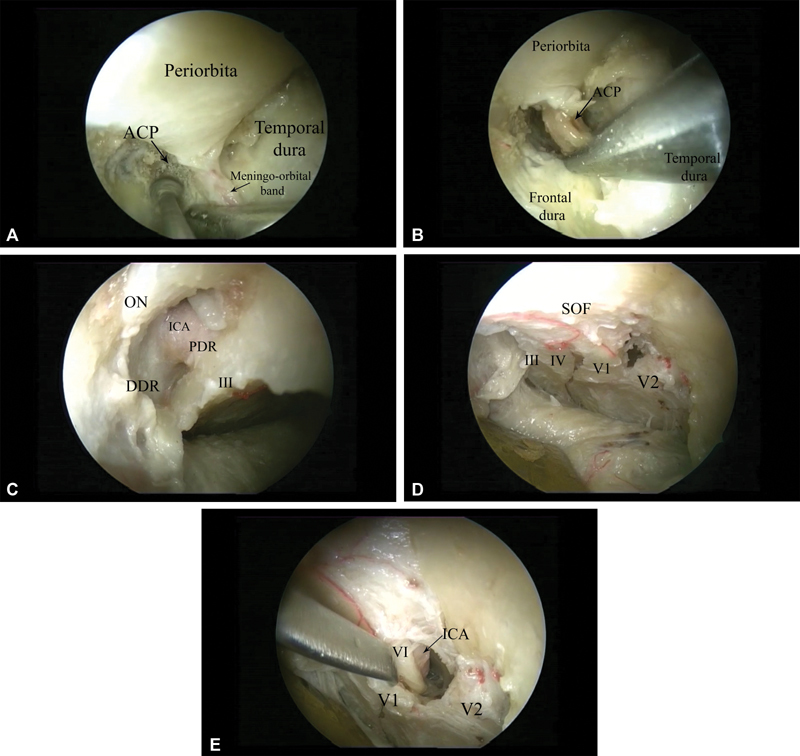
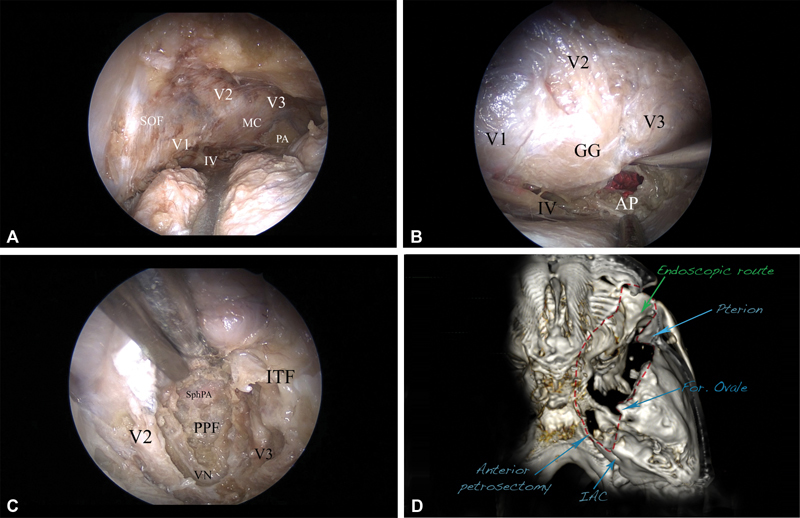
Objective The aim of this anatomic study is to describe a fully endoscopic lateral orbitotomy extradural approach to the cavernous sinus, posterior, and infratemporal fossae. Material and Methods Three prefixed latex-injected head specimens (six orbital exposures) were used in the study. Before and after dissection, a computed tomography scan was performed on each cadaver head and a neuronavigation system was used to guide the approach. The extent of bone removal and the area of exposure of the targeted corridor were evaluated with the aid of OsiriX software (Pixmeo, Bernex, Switzerland). Results The lateral orbital approach offers four main endoscopic extradural routes: the anteromedial, posteromedial, posterior, and inferior. The anteromedial route allows a direct route to the optic canal by removal of the anterior clinoid process, whereas the posteromedial route allows for exposure of the lateral wall of the cavernous sinus. The posterior route is targeted to Meckel's cave and provides access to the posterior cranial fossa by exposure and drilling of the petrous apex, whereas the inferior route gives access to the pterygopalatine and infratemporal fossae by drilling the floor of the middle cranial fossa and the bone between the second and third branches of the trigeminal nerve. Conclusion The lateral orbitotomy endoscopic approach provides direct access to the cavernous sinus, posterior, and infratemporal fossae. Advantages of the approach include a favorable angle of attack, minimal brain retraction, and the possibility of dissection within the two dural layers of the cavernous sinus without entering its neurovascular compartment.
Keywords: anatomy; endoscopic surgery; lateral orbital approach; skull base surgery.
Conflict of interest statement
This article does not contain any studies with human participants performed by any of the authors.
Figures

References
-
- Al-Mefty O. Supraorbital-pterional approach to skull base lesions. Neurosurgery. 1987;21(04):474–477. - PubMed
-
- Hakuba A, Liu S, Nishimura S. The orbitozygomatic infratemporal approach: a new surgical technique. Surg Neurol. 1986;26(03):271–276. - PubMed
-
- Ikeda K, Yamashita J, Hashimoto M, Futami K. Orbitozygomatic temporopolar approach for a high basilar tip aneurysm associated with a short intracranial internal carotid artery: a new surgical approach. Neurosurgery. 1991;28(01):105–110. - PubMed
-
- Jane J A, Park T S, Pobereskin L H, Winn H R, Butler A B. The supraorbital approach: technical note. Neurosurgery. 1982;11(04):537–542. - PubMed
-
- Aziz K M, Froelich S C, Cohen P L, Sanan A, Keller J T, van Loveren H R. The one-piece orbitozygomatic approach: the MacCarty burr hole and the inferior orbital fissure as keys to technique and application. Acta Neurochir (Wien) 2002;144(01):15–24. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
