

EXPRESS: Acute Vasoreactivity Testing in Pediatric Idiopathic Pulmonary Arterial Hypertension: an international Survey on Current Practice
- PMID: 31144586
- PMCID: PMC6886286
- DOI: 10.1177/2045894019857533
EXPRESS: Acute Vasoreactivity Testing in Pediatric Idiopathic Pulmonary Arterial Hypertension: an international Survey on Current Practice
Abstract
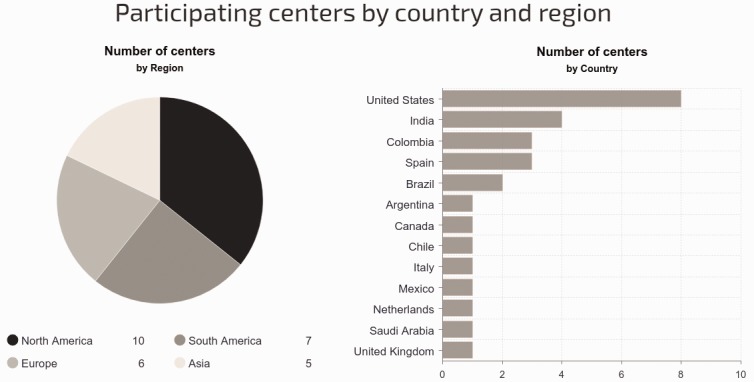
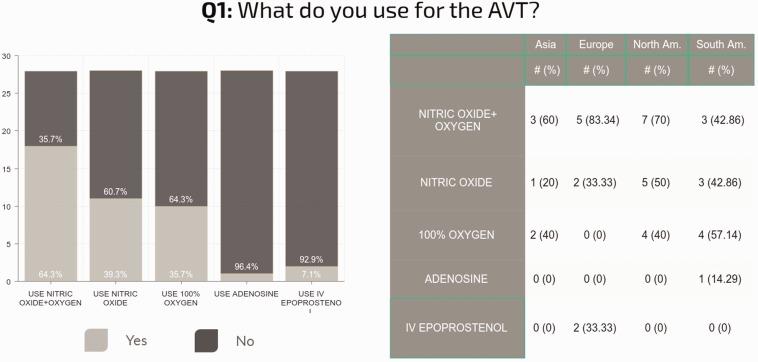
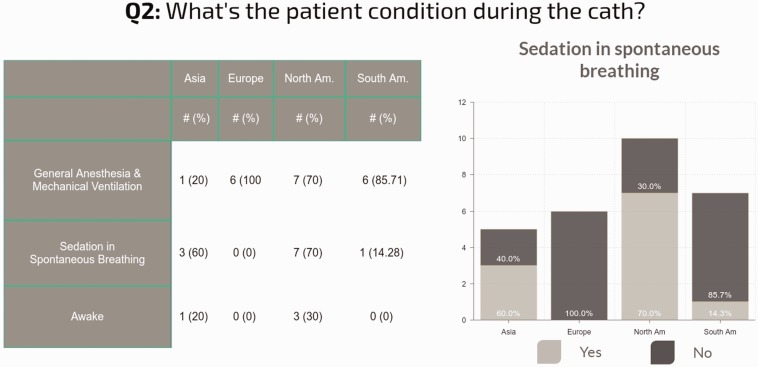
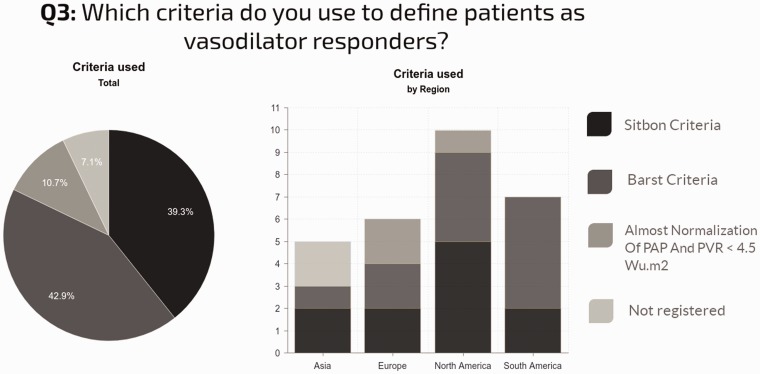
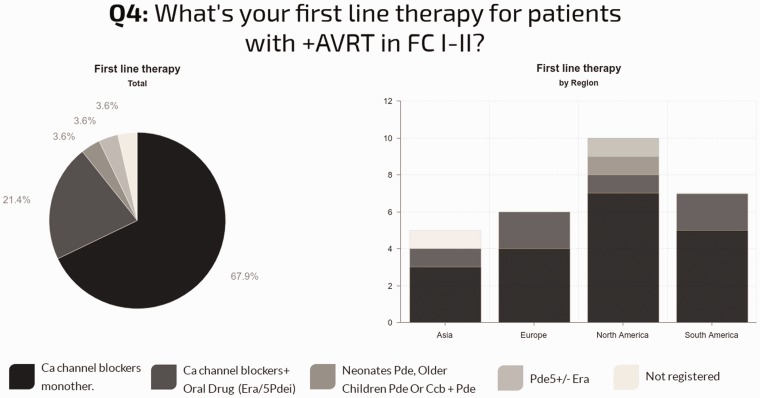
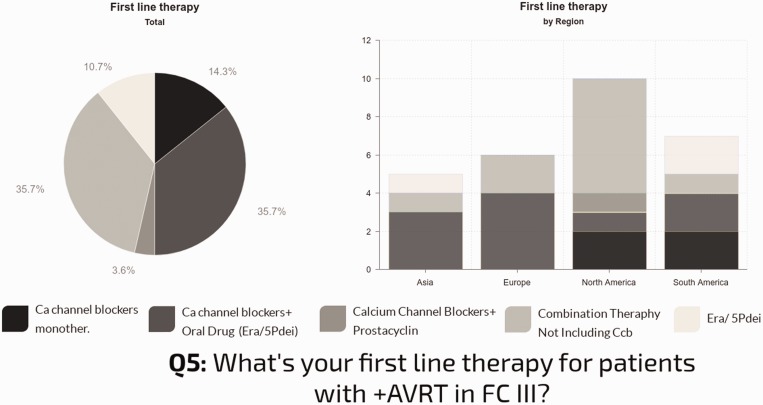
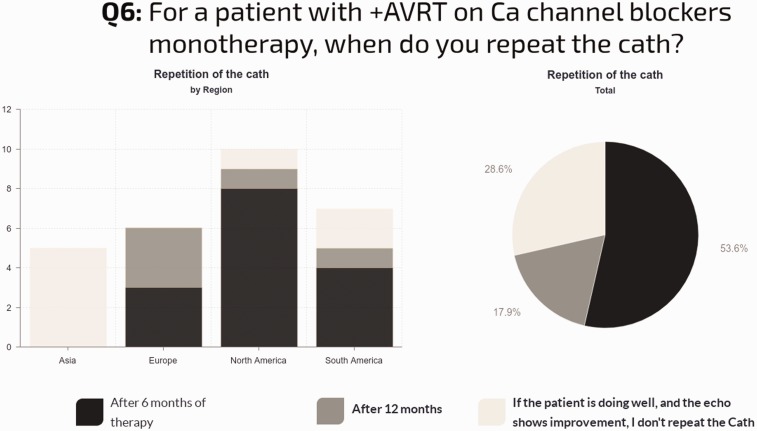
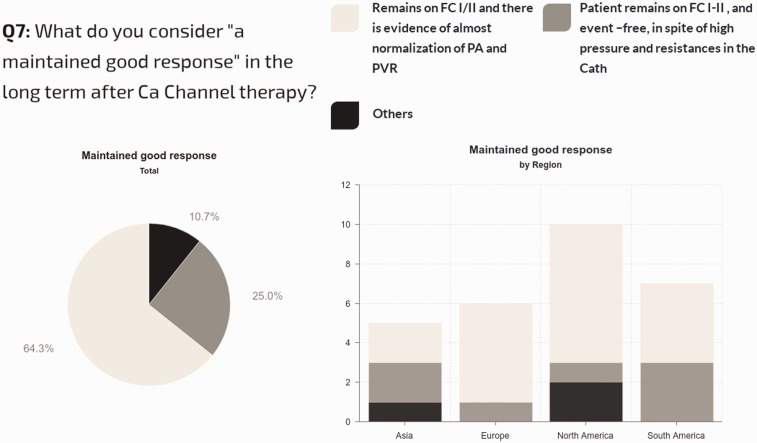
The aim of this study was to determine practice patterns and inter-institutional variability in how acute vasoreactivity testing (AVT) is performed and interpreted in pediatrics throughout the world. A survey was offered to physicians affiliated with the Pediatric & Congenital Heart Disease Taskforce of the Pulmonary Vascular Research Institute (PVRI), the Pediatric Pulmonary Hypertension Network (PPHNET), or the Spanish Registry for Pediatric Pulmonary Hypertension (REHIPED), from February to December 2016. The survey requested data about the site-specific protocol for AVT and subsequent management of pediatric patients with idiopathic pulmonary arterial hypertension (IPAH) or heritable PAH (HPAH). Twenty-eight centers from 13 countries answered the survey. AVT is performed in most centers using inhaled nitric oxide (iNO). Sitbon criteria was used in 39% of the centers, Barst criteria in 43%, and other criteria in 18%. First-line therapy for positive AVT responders in functional class (FC) I/II was calcium channel blocker (CCB) in 89%, but only in 68% as monotherapy. Most centers (71%) re-evaluated AVT-positive patients hemodynamics after 6–12 months; 29% of centers re-evaluated based only on clinical criteria. Most centers (64%) considered a good response as remaining in FC I or II, with near normalization of pulmonary arterial pressure and pulmonary vascular resistance, but a stable FC I/II alone was sufficient criteria in 25% of sites. Protocols and diagnostic criteria for AVT, and therapeutic approaches during follow-up, were highly variable across the world. Reported clinical practice is not fully congruent with current guidelines, suggesting the need for additional studies that better define the prognostic value of AVT for pediatric IPAH patients.
Figures
References
-
- Rich S, Brundage BH, Levy PS. The effect of vasodilator therapy on the clinical outcome of patients with primary pulmonary hypertension. Circulation 1985; 71(6): 1191–1196. - PubMed
-
- Rich S, Brundage BH. High-dose calcium channel-blocking therapy for primary pulmonary hypertension: evidence for long-term reduction in pulmonary arterial pressure and regression of right ventricular hypertrophy. Circulation 1987; 76(1): 135–141. - PubMed
-
- Rich S, Kaufmann E, Levy PS. The effect of high doses of calcium-channel blockers on survival in primary pulmonary hypertension. N Engl J Med 1992; 327: 76–81. - PubMed
-
- Medarov BI, Judson MA. The role of calcium channel blockers for the treatment of pulmonary arterial hypertension: How much do we actually know and how could they be positioned today? Respir Med 2015; 109: 557–564. - PubMed
LinkOut - more resources
Full Text Sources
