

Drug hypersensitivity in HIV infection
- PMID: 31145192
- PMCID: PMC7236403
- DOI: 10.1097/ACI.0000000000000545
Drug hypersensitivity in HIV infection
Abstract
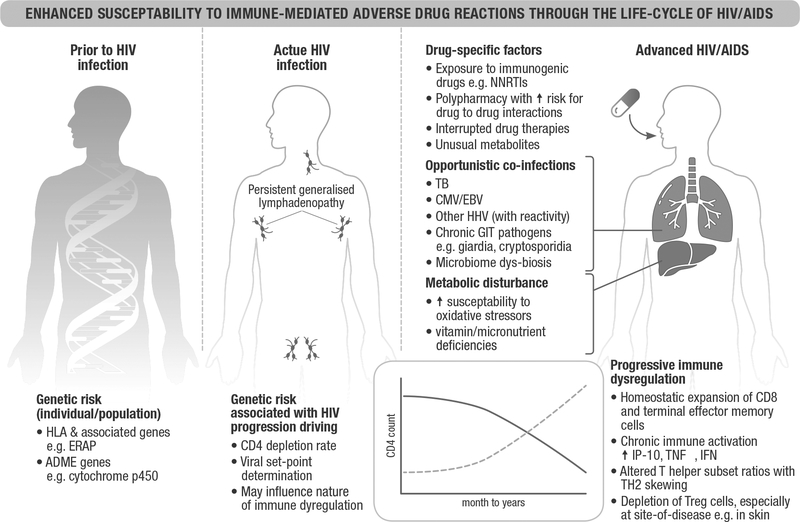
Purpose of review: Immune-mediated adverse drug reactions (IM-ADRs) are many times more common in HIV-infected patients. Usual offending drugs include antiretroviral and antiinfectives, but the burden of specific drug IM-ADRs is population-specific; changing as new and fixed dose combinations enter the market, and drug-resistance patterns demand. This review considers recent literature on epidemiology, mechanisms, clinical management and prevention of IM-ADRs amongst persons living with HIV/AIDS.
Recent findings: Epidemiological studies continue to describe high rates of delayed hypersensitivity to known offenders, as well as similar reactions in preexposure prophylaxis. IM-ADRs to oral and injectable integrase strand transfer inhibitors are reported with expanding use. The clinical spectrum and management of IM-ADRs occurring in HIV-infected populations is similar to uninfected; with exceptions such as a recently described severe delayed efavirenz DILI with high mortality. Furthermore, the context can be unique, such as the lower than expected mortality in a Stevens-Johnson syndrome and toxic epidermal necrolysis (SJS/TEN) cohort from a HIV/TB high burden setting. Programmatic data showing the near complete elimination of Abacavir drug hypersensitivity syndrome following implementation of HLA-B57:01 screening is a stellar example of how prevention is possible with mechanistic insight.
Summary: IM-ADRs remain a challenge in persons living with HIV. The complexities posed by polypharmacy, overlapping drug toxicities, drug interactions, overlap of IM-ADRs with other diseases, limited alternative drugs, and vulnerable patients with advanced immunosuppression with high mortality, necessitate increased use of drug provocation testing, treat-through and desensitization strategies. There is an urgent need for improved diagnostics and predictive biomarkers for prevention, or to guide treat-through, rechallenge and desensitization approaches.
Conflict of interest statement
Conflicts of interest
There are no conflicts of interest.
Figures
References
-
- UNAIDS, Miles to go - Global report and update. UNAIDS, Editor. 2018: Geneva, Switzerland.
-
- Angamo MT, Chalmers L, Curtain CM, et al. Mortality from adverse drug reaction-related hospitalizations in south-west Ethiopia: a cross-sectional study. J Clin Pharm Ther 2018; 43:790–798. - PubMed
-
- Coopman SA, Johnson RA, Platt R, Stern RS. Cutaneous disease and drug reactions in HIV infection. N Engl J Med 1993; 328:1670–1674. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
