

Robot-assisted and laparoscopic vs open radical prostatectomy in clinically localized prostate cancer: perioperative, functional, and oncological outcomes: A Systematic review and meta-analysis
- PMID: 31145297
- PMCID: PMC6709105
- DOI: 10.1097/MD.0000000000015770
Robot-assisted and laparoscopic vs open radical prostatectomy in clinically localized prostate cancer: perioperative, functional, and oncological outcomes: A Systematic review and meta-analysis
Abstract
Background: To perform a systematic review and meta-analysis evaluating the perioperative, functional, and oncological outcomes and cost of robot-assisted radical prostatectomy (RARP), or laparoscopic radical prostatectomy (LRP) comparing with open radical prostatectomy (ORP) in men with clinically localized prostate cancer through all prospective comparative studies.
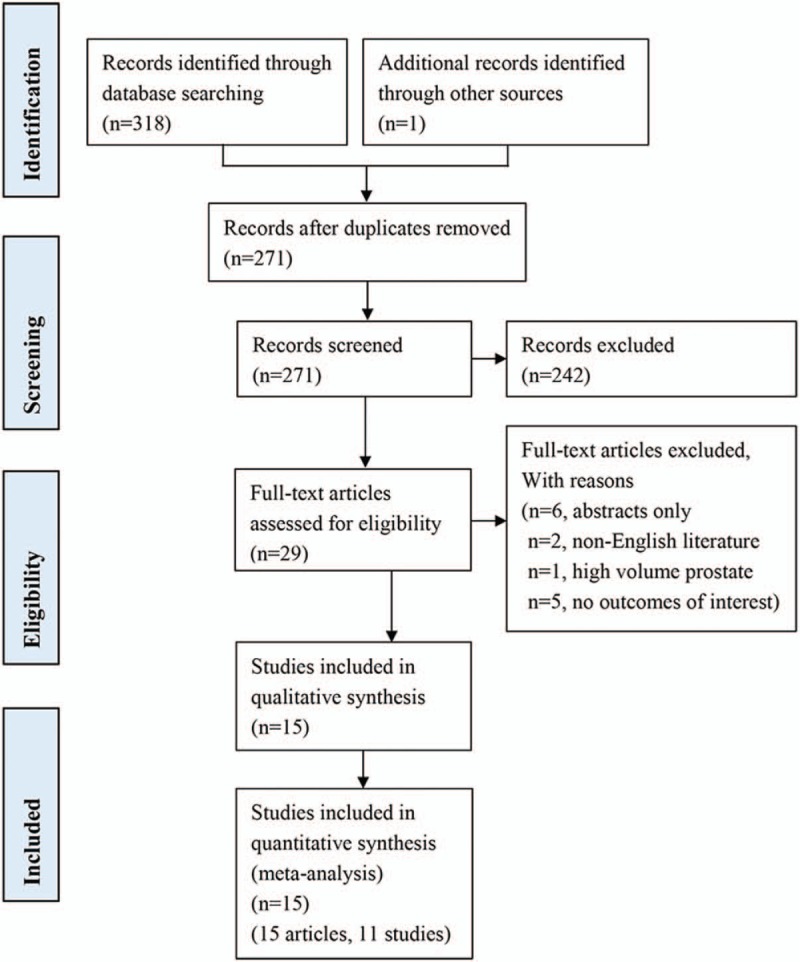
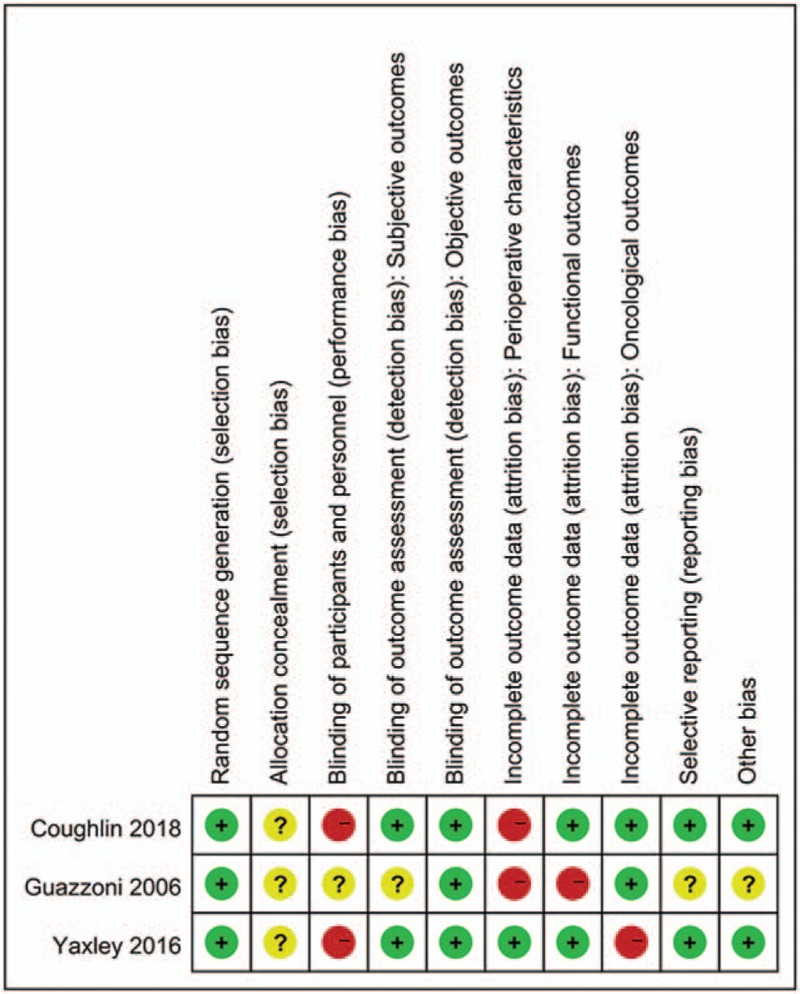
Methods: A comprehensive literature search was performed in August 2018 using the Pubmed, Medline, Embase, and Cochrane databases. Only randomized controlled trials (RCTs) and prospective studies including patients with clinically localized prostate cancer were eligible for study inclusion. Cumulative analysis was conducted using Review Manager v. 5.3 software.
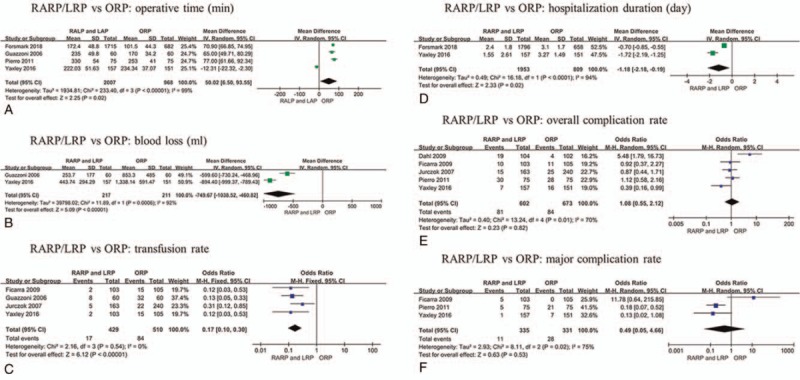
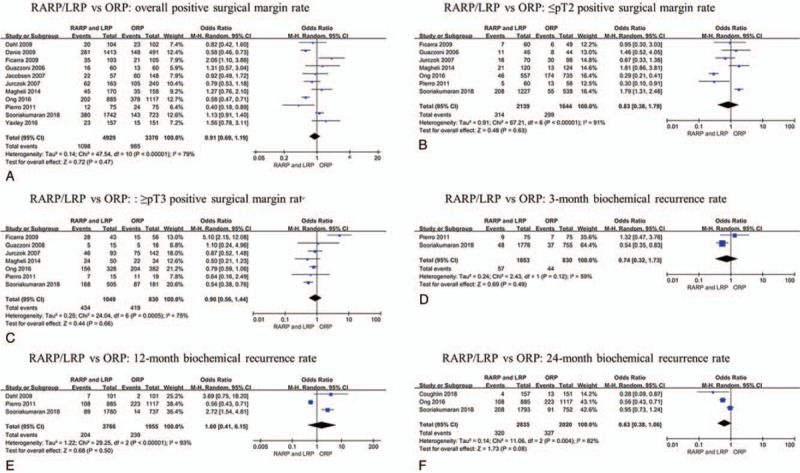
Results: Two RCTs and 9 prospective studies were included in this systematic review. There were no significant differences between RARP/LRP and ORP in overall complication rate, major complication rate, overall positive surgical margin (PSM) rate, ≤pT2 tumor PSM rate, ≥pT3 tumor PSM rate. Moreover, RARP/LRP and ORP showed similarity in biochemical recurrence (BCR) rate at 3, 12, 24 months postoperatively. Urinary continence and erectile function at 12 months postoperatively between RARP and ORP are also comparable. RARP/LRP were associated with significantly lower estimated blood loss [mean difference (MD) -749.67, 95% CI -1038.52 to -460.82, P = .001], lower transfusion rate (OR 0.17, 95% CI 0.10 to 0.30, P < .001) and less hospitalization duration (MD -1.18, 95% CI -2.18 to -0.19, P = .02). And RARP/LRP required more operative time (MD 50.02, 95% CI 6.50 to 93.55, P = .02) and cost.
Conclusion: RARP/LRP is associated with lower blood loss, transfusion rate and less hospitalization duration. The available data were insufficient to prove the superiority of any surgical approach in terms of postoperative complications, functional and oncologic outcomes.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures

References
-
- Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018;68:394–424. - PubMed
-
- Wong MC, Goggins WB, Wang HH, et al. Global incidence and mortality for prostate cancer: analysis of temporal patterns and trends in 36 countries. Eur Urol 2016;70:862–74. - PubMed
-
- Sanda MG, Cadeddu JA, Kirkby E, et al. Clinically localized prostate cancer: AUA/ASTRO/SUO Guideline. Part II: recommended approaches and details of specific care options. J Urol 2018;199:990–7. - PubMed
-
- Mottet N, Bellmunt J, Bolla M, et al. EAU-ESTRO-SIOG Guidelines on Prostate Cancer. Part 1: screening, diagnosis, and local treatment with curative intent. Eur Urol 2017;71:618–29. - PubMed
-
- Raboy A, Ferzli G, Albert P. Initial experience with extraperitoneal endoscopic radical retropubic prostatectomy. Urology 1997;50:849–53. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
