

Burden and Outcomes of Heart Failure Hospitalizations in Adults With Chronic Kidney Disease
- PMID: 31146814
- PMCID: PMC6590908
- DOI: 10.1016/j.jacc.2019.02.071
Burden and Outcomes of Heart Failure Hospitalizations in Adults With Chronic Kidney Disease
Abstract
Background: Data on rates of heart failure (HF) hospitalizations, recurrent hospitalizations, and outcomes related to HF hospitalizations in chronic kidney disease (CKD) are limited.
Objectives: This study examined rates of HF hospitalizations and re-hospitalizations within a large CKD population and evaluated the burden of HF hospitalizations with the risk of subsequent CKD progression and death.
Methods: The prospective CRIC (Chronic Renal Insufficiency Cohort) study measured the estimated glomerular filtration rate (eGFR) and urine albumin-to-creatinine ratio (ACR) at baseline. The crude rates and rate ratios of HF hospitalizations and 30-day HF re-hospitalizations were calculated using Poisson regression models. Cox regression was used to assess the association of the frequency of HF hospitalizations within the first 2 years of follow-up with risk of subsequent CKD progression and death.
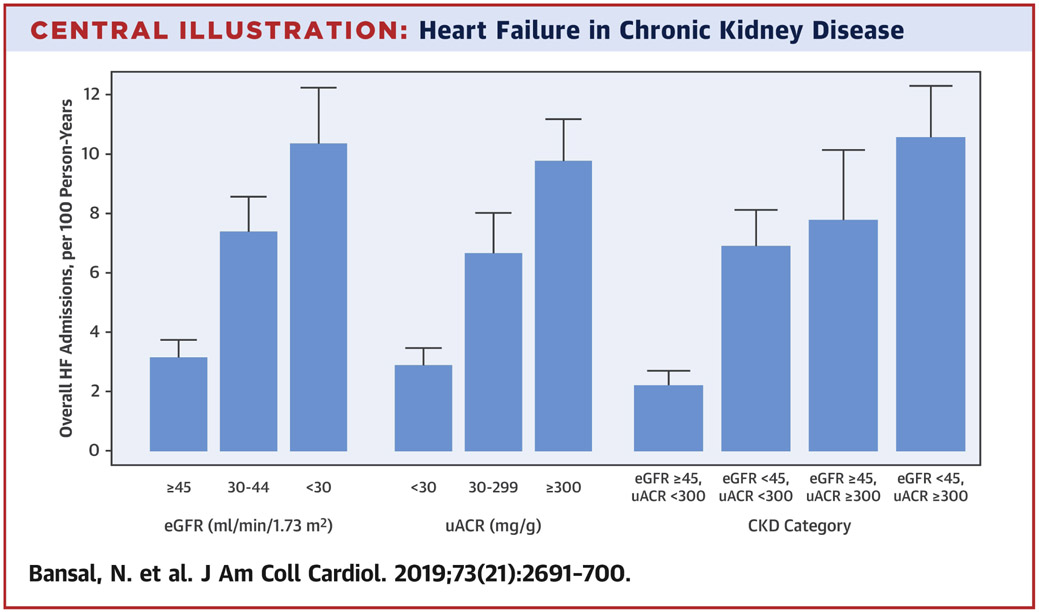
Results: Among 3,791 participants, the crude rate of HF admissions was 5.8 per 100 person-years (with higher rates of HF with preserved ejection fraction vs. HF with reduced ejection fraction). The adjusted rate of HF was higher with a lower eGFR (vs. eGFR >45 ml/min/1.73 m2); the rate ratios were 1.7 and 2.2 for eGFR 30 to 44 and <30 ml/min/1.73 m2 (vs. >45 ml/min/1.73 m2), respectively. Similarly, the adjusted rates of HF hospitalization were significantly higher in those with higher urine ACR (vs. urine ACR <30 mg/g); the rate ratios were 1.9 and 2.6 for urine ACR 30 to 299 and ≥300 mg/g, respectively. Overall, 20.6% of participants had a subsequent HF re-admission within 30 days. HF hospitalization within 2 years of study entry was associated with greater adjusted risks for CKD progression (1 hospitalization: hazard ratio [HR]: 1.93; 95% confidence interval [CI]: 1.40 to 2.67; 2+ hospitalizations: HR: 2.14; 95% CI: 1.30 to 3.54) and all-cause death (1 hospitalization: HR: 2.20; 95% CI: 1.71 to 2.84; 2+ hospitalizations: HR: 3.06; 95% CI: 2.23 to 4.18).
Conclusions: Within a large U.S. CKD population, the rates of HF hospitalizations and re-hospitalization were high, with even higher rates across categories of lower eGFR and higher urine ACR. Patients with CKD hospitalized with HF had greater risks of CKD progression and death. HF prevention and treatment should be a public health priority to improve CKD outcomes.
Keywords: chronic kidney disease; end-stage renal-disease; heart failure; mortality; outcomes.
Copyright © 2019 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Congestive Heart Failure and Chronic Kidney Disease: The CardioRenal/NephroCardiology Connection.J Am Coll Cardiol. 2019 Jun 4;73(21):2701-2704. doi: 10.1016/j.jacc.2019.03.474. J Am Coll Cardiol. 2019. PMID: 31146815 No abstract available.
References
-
- Giamouzis G, Kalogeropoulos A, Georgiopoulou V et al. Hospitalization epidemic in patients with heart failure: risk factors, risk prediction, knowledge gaps, and future directions. J Card Fail 2011;17:54–75. - PubMed
-
- Kociol RD, Hammill BG, Fonarow GC et al. Generalizability and longitudinal outcomes of a national heart failure clinical registry: Comparison of Acute Decompensated Heart Failure National Registry (ADHERE) and non-ADHERE Medicare beneficiaries. Am Heart J 2010;160:885–92. - PubMed
Publication types
MeSH terms
Grants and funding
- R01 DK072231/DK/NIDDK NIH HHS/United States
- UL1 TR002548/TR/NCATS NIH HHS/United States
- U01 DK060980/DK/NIDDK NIH HHS/United States
- U01 DK060963/DK/NIDDK NIH HHS/United States
- UL1 RR024131/RR/NCRR NIH HHS/United States
- M01 RR013987/RR/NCRR NIH HHS/United States
- UL1 TR000003/TR/NCATS NIH HHS/United States
- UL1 TR000439/TR/NCATS NIH HHS/United States
- U01 DK060990/DK/NIDDK NIH HHS/United States
- UL1 TR002240/TR/NCATS NIH HHS/United States
- L30 DK110819/DK/NIDDK NIH HHS/United States
- P30 DK092949/DK/NIDDK NIH HHS/United States
- UL1 RR029879/RR/NCRR NIH HHS/United States
- U01 DK061028/DK/NIDDK NIH HHS/United States
- UL1 TR000433/TR/NCATS NIH HHS/United States
- U01 DK060984/DK/NIDDK NIH HHS/United States
- U01 DK061021/DK/NIDDK NIH HHS/United States
- U01 DK061022/DK/NIDDK NIH HHS/United States
- R01 DK103612/DK/NIDDK NIH HHS/United States
- UL1 TR000424/TR/NCATS NIH HHS/United States
- R01 HL141846/HL/NHLBI NIH HHS/United States
- M01 RR016500/RR/NCRR NIH HHS/United States
- P20 GM109036/GM/NIGMS NIH HHS/United States
- U01 DK060902/DK/NIDDK NIH HHS/United States
- UL1 TR002003/TR/NCATS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
