

Survival and patient-centered outcome in a disease-based observational cohort study of patients with thoracoabdominal aortic aneurysm
- PMID: 31147133
- PMCID: PMC7064148
- DOI: 10.1016/j.jvs.2019.02.033
Survival and patient-centered outcome in a disease-based observational cohort study of patients with thoracoabdominal aortic aneurysm
Abstract
Background: Much of the literature describing treatment for thoracoabdominal aortic aneurysm (TAAA) consists of operative series reported by centers of excellence. These studies are limited by referral and selection bias and exclude patients who are not candidates for the reported modality of repair. Little is known about the patients who are not referred or selected for repair. For those undergoing intervention, outcomes such as functional status after surgery are rarely reported. In this study, we address these gaps by reporting two primary end points: 1-year survival and a "good" outcome (defined as successful aneurysm exclusion, freedom from permanent loss of organ system function, and return to preoperative functional status after surgery) in a cohort of TAAA patients, including all nonoperative and operative patients, irrespective of treatment modality.
Methods: A single-institution database was screened by diagnosis codes for TAAA from 2009 to 2017 using the International Classification of Diseases versions 9 and 10. Diagnosis was confirmed by retrospective chart review and computed tomography findings of aneurysmal degeneration ≥3.2 cm of the paravisceral aorta in continuity with aneurysmal aorta meeting standard criteria for repair. Patients <18 years of age and those with mycotic aneurysm were excluded. Patients were either managed nonoperatively or by one of four operative strategies: (i) open; (ii) endovascular with branched endografts; (iii) hybrid, defined as iliovisceral debranching followed by endograft placement; or (iv) partial repair in which the paravisceral segment was intentionally left unaddressed.
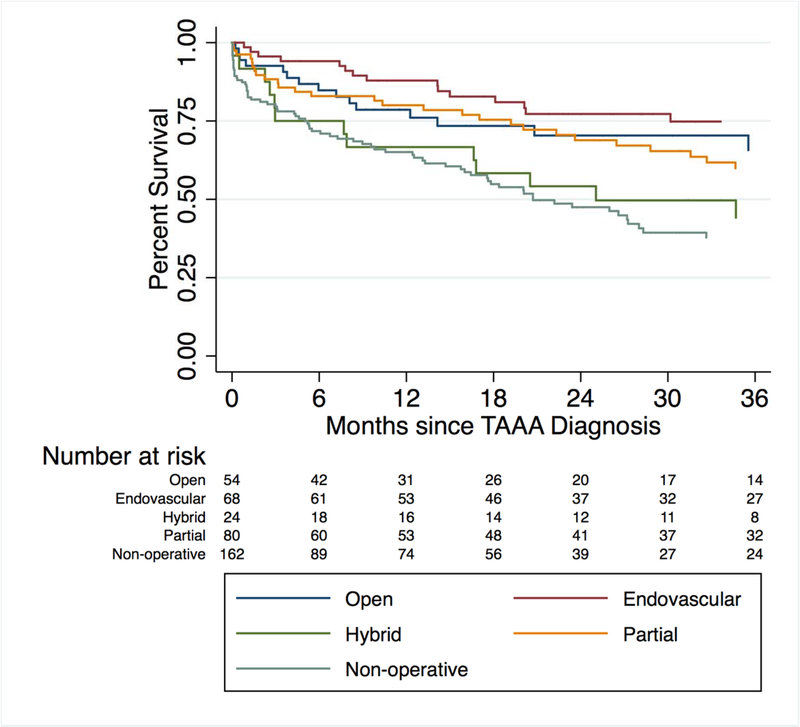
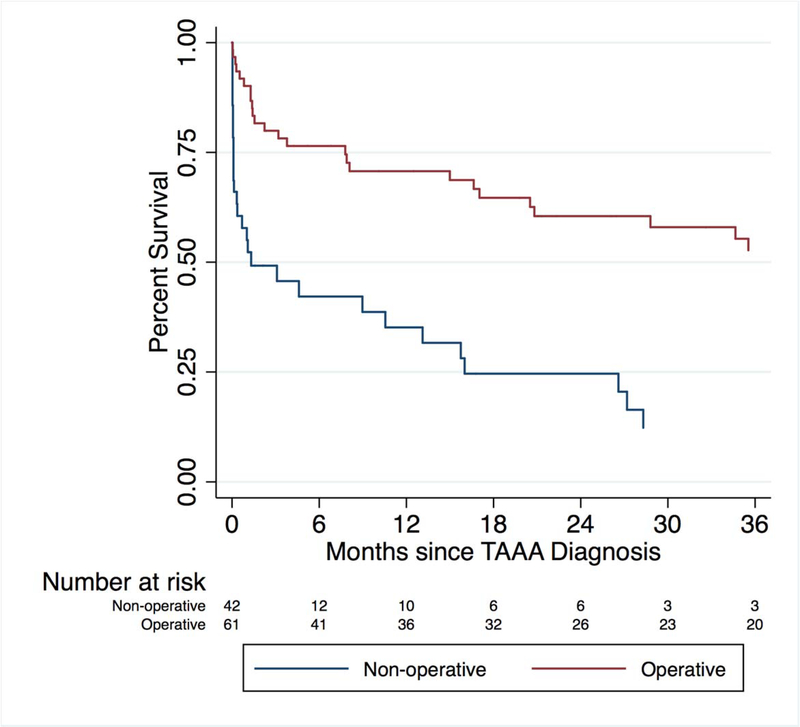
Results: Among the entire cohort of 432 patients with TAAA, significant comorbidities were seen in 143 (33%). Forty-seven percent of the patients were managed nonoperatively. Of these, 65% survived to 1 year. A survival benefit was seen in the open, endovascular, and partial, but not hybrid, operative groups compared with the nonoperative group during a 3-year period. Overall 1-year survival was 81%, but only 65% had a good outcome (P = .0016).
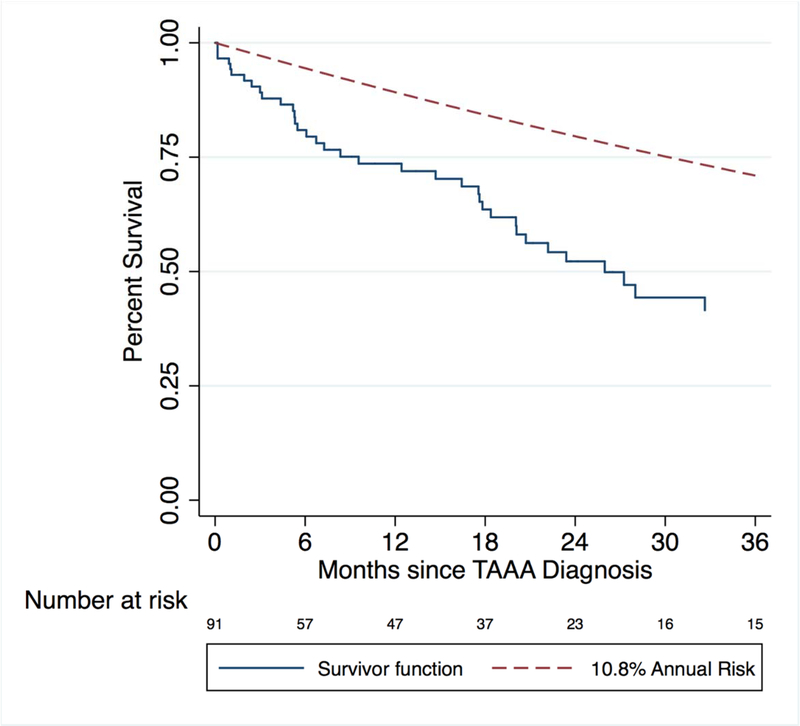
Conclusions: Nearly half of the patients in this inclusive cohort study did not undergo repair despite access to a variety of operative techniques. Many of these patients die in the short term due to high burden of comorbid disease rather than aneurysm rupture. Among those undergoing operation, a notable difference between survival and good outcome was observed. Operation appears to confer a survival advantage among appropriately selected patients with TAAA, but a large proportion are high risk and may not benefit from operative repair due to limited baseline survival and lower probability of good outcome.
Keywords: Aortic aneurysm; Complex endovascular aneurysm repair; Hybrid aneurysm repair; Nonoperative management; Open thoracoabdominal aneurysm repair; Thoracoabdominal aortic aneurysm.
Copyright © 2019 Society for Vascular Surgery. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Elefteriades JA. Natural history of thoracic aortic aneurysms: indications for surgery, and surgical versus nonsurgical risks. Ann Thorac Surg. 2002;74(5):S1877–80; discussion S1892–8. http://www.ncbi.nlm.nih.gov/pubmed/12440685. Accessed April 8, 2017. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
