

Source attribution of Campylobacter jejuni shows variable importance of chicken and ruminants reservoirs in non-invasive and invasive French clinical isolates
- PMID: 31147581
- PMCID: PMC6542803
- DOI: 10.1038/s41598-019-44454-2
Source attribution of Campylobacter jejuni shows variable importance of chicken and ruminants reservoirs in non-invasive and invasive French clinical isolates
Abstract
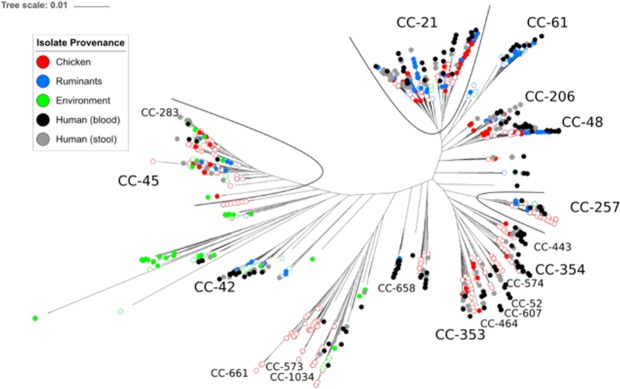
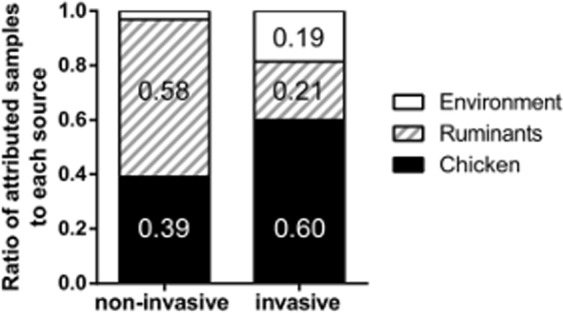
Campylobacter jejuni is the most common cause of bacterial gastroenteritis worldwide. Mainly isolated from stool samples, C. jejuni can also become invasive. C. jejuni belongs to the commensal microbiota of a number of hosts, and infection by this bacterium can sometimes be traced back to exposure to a specific source. Here we genome sequenced 200 clinical isolates (2010-2016) and analyzed them with 701 isolate genomes from human infection, chicken, ruminants and the environment to examine the relative contribution of different reservoirs to non-invasive and invasive infection in France. Host-segregating genetic markers that can discriminate C. jejuni source were used with STRUCTURE software to probabilistically attribute the source of clinical strains. A self-attribution correction step, based upon the accuracy of source apportionment within each potential reservoir, improved attribution accuracy of clinical strains and suggested an important role for ruminant reservoirs in non-invasive infection and a potentially increased contribution of chicken as a source of invasive isolates. Structured sampling of Campylobacter in the clinic and from potential reservoirs provided evidence for variation in the contribution of different infection sources over time and an important role for non-poultry reservoirs in France. This provides a basis for ongoing genomic epidemiology surveillance and targeted interventions.
Conflict of interest statement
The authors declare no competing interests.
Figures


References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
