

Amustaline-glutathione pathogen-reduced red blood cell concentrates for transfusion-dependent thalassaemia
- PMID: 31148155
- PMCID: PMC6771954
- DOI: 10.1111/bjh.15963
Amustaline-glutathione pathogen-reduced red blood cell concentrates for transfusion-dependent thalassaemia
Abstract
Transfusion-dependent thalassaemia (TDT) requires red blood cell concentrates (RBCC) to prevent complications of anaemia, but carries risk of infection. Pathogen reduction of RBCC offers potential to reduce infectious risk. We evaluated the efficacy and safety of pathogen-reduced (PR) Amustaline-Glutathione (A-GSH) RBCC for TDT. Patients were randomized to a blinded 2-period crossover treatment sequence for six transfusions over 8-10 months with Control and A-GSH-RBCC. The efficacy outcome utilized non-inferiority analysis with 90% power to detect a 15% difference in transfused haemoglobin (Hb), and the safety outcome was the incidence of antibodies to A-GSH-PR-RBCC. By intent to treat (80 patients), 12·5 ± 1·9 RBCC were transfused in each period. Storage durations of A-GSH and C-RBCC were similar (8·9 days). Mean A-GSH-RBCC transfused Hb (g/kg/day) was not inferior to Control (0·113 ± 0·04 vs. 0·111 ± 0·04, P = 0·373, paired t-test). The upper bound of the one-sided 95% confidence interval for the treatment difference from the mixed effects model was 0·005 g/kg/day, within a non-inferiority margin of 0·017 g/kg/day. A-GSH-RBCC mean pre-transfusion Hb levels declined by 6·0 g/l. No antibodies to A-GSH-RBCC were detected, and there were no differences in adverse events. A-GSH-RBCCs offer potential to reduce infectious risk in TDT with a tolerable safety profile.
Keywords: RBC; infection; iron; thalassaemia; transfusion.
© 2019 The Authors. British Journal of Haematology published by British Society for Haematology and John Wiley & Sons Ltd.
Conflict of interest statement
Yesim Aydinok, Antonio Piga, and Rafaella Origa received institutional research support from Cerus for conduct of the study. Nina Mufti, Anna Erickson, Anne North, Katie Waldhaus, Christine Ernst, Jin‐Sying Lin, Norman Huang, Richard J. Benjamin, and Laurence Corash were employees of Cerus Corporation and beneficial owners of Cerus stock and/or stock options during the conduct of the study and the preparation of the manuscript. The INTERCEPT Blood System for Red Blood Cells and Amustaline‐Glutathione RBCC are not FDA licensed.
Figures



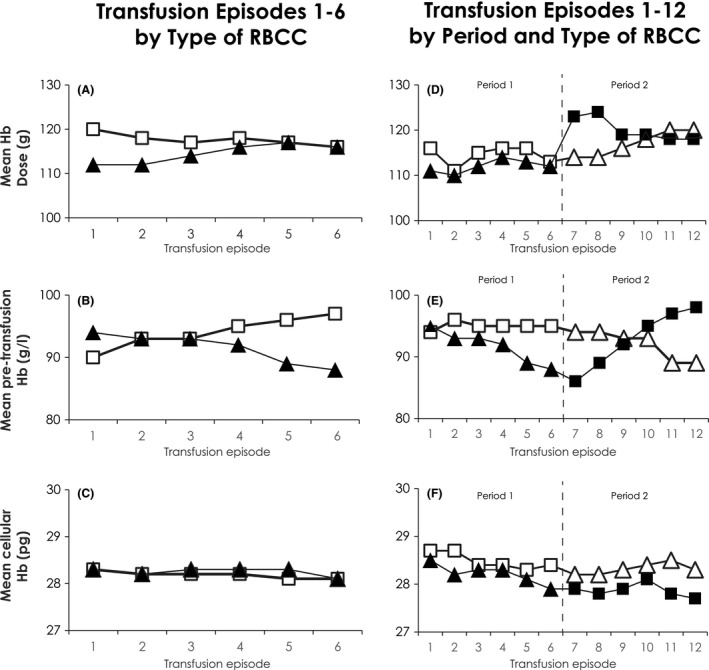
 ) red blood cell concentrate (
) red blood cell concentrate ( ) for episodes 7–12. For 39 patients, Control
) for episodes 7–12. For 39 patients, Control  ) were transfused in Period 1 for episodes 1–6 followed by Test
) were transfused in Period 1 for episodes 1–6 followed by Test  ) in Period 2 for episodes 7–12. (D) Mean Hb dose (g) transfused per episode; (E) Mean pre‐transfusion patient Hb (g/l) per episode; (F) Pre‐transfusion patient
) in Period 2 for episodes 7–12. (D) Mean Hb dose (g) transfused per episode; (E) Mean pre‐transfusion patient Hb (g/l) per episode; (F) Pre‐transfusion patient References
-
- Al‐Riyami, A.Z. , Al‐Muqbali, A. , Al‐Sudiri, S. , Murthi Panchatcharam, S. , Zacharia, M. , Al‐Mahrooqi, S. , Al‐Hosni, S. , Al‐Marhoobi, A. & Daar, S. (2018) Risks of red blood cell alloimmunization in transfusion‐dependent beta‐thalassemia in Oman: a 25‐year experience of a University Tertiary Care Reference Center and a literature review. Transfusion, 58, 871–878. - PubMed
-
- Benjamin, R.J. , McCullough, J. , Mintz, P.D. , Snyder, E. , Spotnitz, W.D. , Rizzo, R.J. , Wages, D. , Lin, J.S. , Wood, L. , Corash, L. & Conlan, M.G. (2005) Therapeutic efficacy and safety of red blood cells treated with a chemical process (S‐303) for pathogen inactivation: a phase III clinical trial in cardiac surgery patients. Transfusion, 45, 1739–1749. - PubMed
-
- Brixner, V. , Kiessling, A.H. , Madlener, K. , Muller, M.M. , Leibacher, J. , Dombos, S. , Weber, I. , Pfeiffer, H.U. , Geisen, C. , Schmidt, M. , Henschler, R. , North, A. , Huang, N. , Mufti, N. , Erickson, A. , Ernst, C. , Rico, S. , Benjamin, R.J. , Corash, L.M. & Seifried, E. (2018) Red blood cells treated with the amustaline (S‐303) pathogen reduction system: a transfusion study in cardiac surgery. Transfusion, 58, 905–916. - PubMed
-
- Cancelas, J.A. , Gottschall, J.L. , Rugg, N. , Graminske, S. , Schott, M.A. , North, A. , Huang, N. , Mufti, N. , Erickson, A. , Rico, S. & Corash, L. (2017) Red blood cell concentrates treated with the amustaline (S‐303) pathogen reduction system and stored for 35 days retain post‐transfusion viability: results of a two‐centre study. Vox Sanguinis, 112, 210–218. - PubMed
-
- Candotti, D. , Assennato, S.M. , Laperche, S. , Allain, J.P. & Levicnik‐Stezinar, S. (2019) Multiple HBV transfusion transmissions from undetected occult infections: revising the minimal infectious dose. Gut, 68, 313–321. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
